Delfino Ralph J, Staimer Norbert, Tjoa Thomas, Gillen Daniel L, Polidori Andrea, Arhami Mohammad, Kleinman Micheal T, Vaziri Nosratola D, Longhurst John, Sioutas Constantinos
Department of Epidemiology, School of Medicine, University of California, Irvine, Irvine, California 92617, USA.
Environ Health Perspect. 2009 Aug;117(8):1232-8. doi: 10.1289/ehp.0800194. Epub 2009 Apr 29.
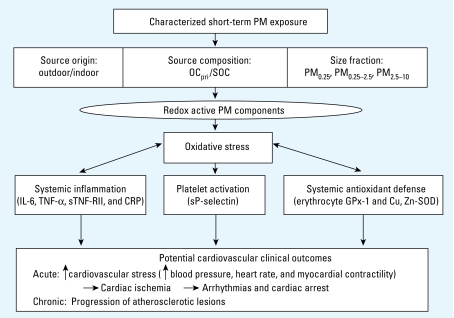
Mechanisms involving oxidative stress and inflammation have been proposed to explain associations of ambient air pollution with cardiovascular morbidity and mortality. Experimental evidence suggests that organic components and ultrafine particles (UFP) are important.
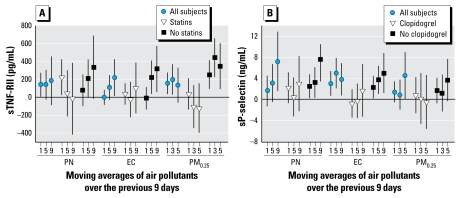
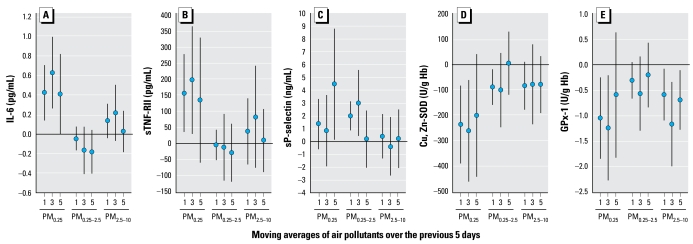
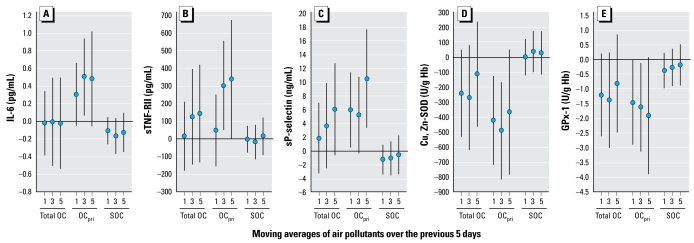
We conducted a panel study of 60 elderly subjects with coronary artery disease living in retirement communities within the Los Angeles, California, air basin. Weekly biomarkers of inflammation included plasma interleukin-6, tumor necrosis factor-alpha soluble receptor II (sTNF-RII), soluble platelet selectin (sP-selectin), and C-reactive protein (CRP). Biomarkers of erythrocyte antioxidant activity included glutathione peroxidase-1 and superoxide dismutase. Exposures included outdoor home daily particle mass [particulate matter < 0.25, 0.25-2.5, and 2.5-10 microm in aerodynamic diameter (PM(0.25), PM(0.25-2.5), PM(2.5-10))], and hourly elemental and black carbon (EC-BC), estimated primary and secondary organic carbon (OC(pri), SOC), particle number (PN), carbon monoxide (CO), and nitrogen oxides-nitrogen dioxide (NO(x)-NO(2)). We analyzed the relation of biomarkers to exposures with mixed effects models adjusted for potential confounders.
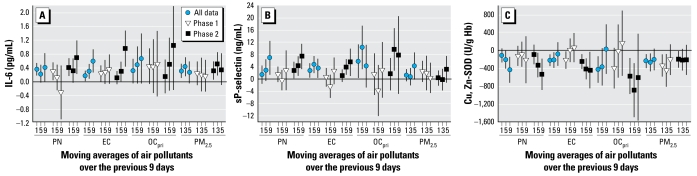
Primary combustion markers (EC-BC, OC(pri), CO, NO(x)-NO(2)), but not SOC, were positively associated with inflammatory biomarkers and inversely associated with erythrocyte anti-oxidant enzymes (n = 578). PN and PM(0.25) were more strongly associated with biomarkers than PM(0.25-2.5). Associations for all exposures were stronger during cooler periods when only OC(pri), PN, and NO(x) were higher. We found weaker associations with statin (sTNF-RII, CRP) and clopidogrel use (sP-selectin).
Traffic-related air pollutants are associated with increased systemic inflammation, increased platelet activation, and decreased erythrocyte antioxidant enzyme activity, which may be partly behind air pollutant-related increases in systemic inflammation. Differences in association by particle size, OC fraction, and seasonal period suggest components carried by UFP are important.
涉及氧化应激和炎症的机制已被提出用于解释环境空气污染与心血管发病率和死亡率之间的关联。实验证据表明有机成分和超细颗粒物(UFP)很重要。
我们对居住在加利福尼亚州洛杉矶空气流域退休社区的60名老年冠心病患者进行了一项队列研究。炎症的每周生物标志物包括血浆白细胞介素-6、肿瘤坏死因子-α可溶性受体II(sTNF-RII)、可溶性血小板选择素(sP-选择素)和C反应蛋白(CRP)。红细胞抗氧化活性的生物标志物包括谷胱甘肽过氧化物酶-1和超氧化物歧化酶。暴露因素包括室外家庭每日颗粒物质量[空气动力学直径<0.25、0.25 - 2.5和2.5 - 10微米的颗粒物(PM(0.25)、PM(0.25 - 2.5)、PM(2.5 - 10))],以及每小时的元素碳和黑碳(EC - BC)、估计的一次和二次有机碳(OC(pri)、SOC)、颗粒数(PN)、一氧化碳(CO)和氮氧化物 - 二氧化氮(NO(x) - NO(2))。我们使用针对潜在混杂因素进行调整的混合效应模型分析了生物标志物与暴露因素之间的关系。
一次燃烧标志物(EC - BC、OC(pri)、CO、NO(x) - NO(2)),而非SOC,与炎症生物标志物呈正相关,与红细胞抗氧化酶呈负相关(n = 578)。PN和PM(0.25)与生物标志物的关联比PM(0.25 - 2.5)更强。在较冷时期,当仅OC(pri)、PN和NO(x)较高时,所有暴露因素的关联更强。我们发现使用他汀类药物(sTNF - RII、CRP)和氯吡格雷(sP - 选择素)时关联较弱。
与交通相关的空气污染物与全身炎症增加、血小板活化增加以及红细胞抗氧化酶活性降低有关,这可能是空气污染相关全身炎症增加的部分原因。粒径、OC组分和季节期间的关联差异表明UFP携带的成分很重要。