Scherr Daniel, Kastner Peter, Kollmann Alexander, Hallas Andreas, Auer Johann, Krappinger Heinz, Schuchlenz Herwig, Stark Gerhard, Grander Wilhelm, Jakl Gabriele, Schreier Guenter, Fruhwald Friedrich M
Department of Cardiology, Medical University Graz, Graz, Austria.
J Med Internet Res. 2009 Aug 17;11(3):e34. doi: 10.2196/jmir.1252.
Telemonitoring of patients with chronic heart failure (CHF) is an emerging concept to detect early warning signs of impending acute decompensation in order to prevent hospitalization.
The goal of the MOBIle TELemonitoring in Heart Failure Patients Study (MOBITEL) was to evaluate the impact of home-based telemonitoring using Internet and mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation.
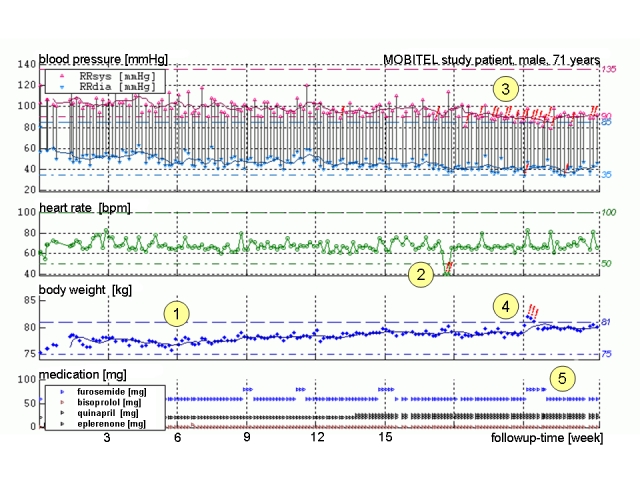
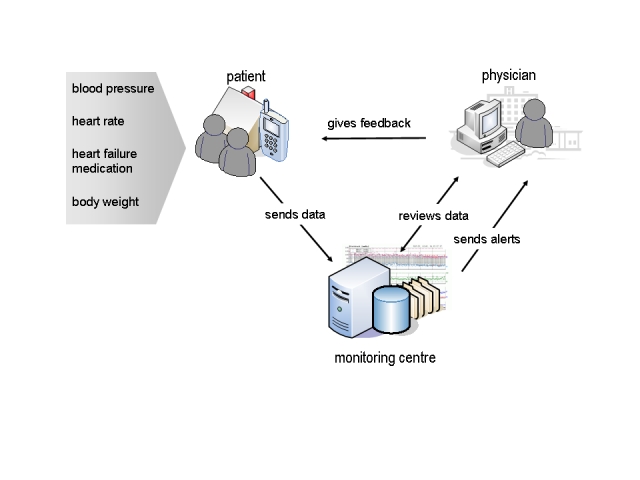
Patients were randomly allocated to pharmacological treatment (control group) or to pharmacological treatment with telemedical surveillance for 6 months (tele group). Patients randomized into the tele group were equipped with mobile phone-based patient terminals for data acquisition and data transmission to the monitoring center. Study physicians had continuous access to the data via a secure Web portal. If transmitted values went outside individually adjustable borders, study physicians were sent an email alert. Primary endpoint was hospitalization for worsening CHF or death from cardiovascular cause.
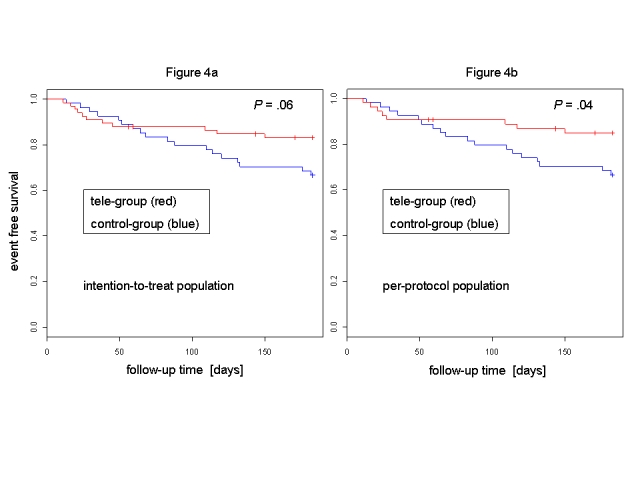
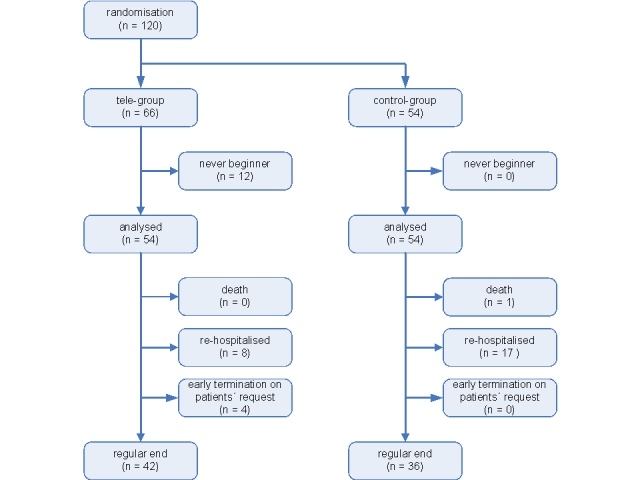
The study was stopped after randomization of 120 patients (85 male, 35 female); median age was 66 years (IQR 62-72). The control group comprised 54 patients (39 male, 15 female) with a median age of 67 years (IQR 61-72), and the tele group included 54 patients (40 male, 14 female) with a median age of 65 years (IQR 62-72). There was no significant difference between groups with regard to baseline characteristics. Twelve tele group patients were unable to begin data transmission due to the inability of these patients to properly operate the mobile phone ("never beginners"). Four patients did not finish the study due to personal reasons. Intention-to-treat analysis at study end indicated that 18 control group patients (33%) reached the primary endpoint (1 death, 17 hospitalizations), compared with 11 tele group patients (17%, 0 deaths, 11 hospitalizations; relative risk reduction 50%, 95% CI 3-74%, P = .06). Per-protocol analysis revealed that 15% of tele group patients (0 deaths, 8 hospitalizations) reached the primary endpoint (relative risk reduction 54%, 95% CI 7-79%, P= .04). NYHA class improved by one class in tele group patients only (P< .001). Tele group patients who were hospitalized for worsening heart failure during the study had a significantly shorter length of stay (median 6.5 days, IQR 5.5-8.3) compared with control group patients (median 10.0 days, IQR 7.0-13.0; P= .04). The event rate of never beginners was not higher than the event rate of control group patients.
Telemonitoring using mobile phones as patient terminals has the potential to reduce frequency and duration of heart failure hospitalizations. Providing elderly patients with an adequate user interface for daily data acquisition remains a challenging component of such a concept.
对慢性心力衰竭(CHF)患者进行远程监测是一个新兴概念,旨在检测即将发生急性失代偿的早期预警信号,以预防住院治疗。
心力衰竭患者移动远程监测研究(MOBITEL)的目标是评估使用互联网和移动电话技术进行家庭远程监测对急性失代偿发作后心力衰竭患者预后的影响。
患者被随机分配至药物治疗组(对照组)或接受为期6个月的远程医疗监测的药物治疗组(远程监测组)。随机进入远程监测组的患者配备了基于移动电话的患者终端,用于数据采集并将数据传输至监测中心。研究医生可通过安全的网络门户持续访问数据。如果传输值超出个体可调整范围,会向研究医生发送电子邮件警报。主要终点是因CHF恶化住院或心血管原因死亡。
在120例患者(85例男性,35例女性)随机分组后,研究停止;中位年龄为66岁(四分位间距62 - 72岁)。对照组包括54例患者(39例男性,15例女性),中位年龄为67岁(四分位间距61 - 72岁),远程监测组包括54例患者(40例男性,14例女性),中位年龄为65岁(四分位间距62 - 72岁)。两组在基线特征方面无显著差异。12例远程监测组患者因无法正确操作移动电话(“从未使用者”)而无法开始数据传输。4例患者因个人原因未完成研究。研究结束时的意向性分析表明,18例对照组患者(33%)达到主要终点(1例死亡,17例住院),相比之下,11例远程监测组患者(17%,0例死亡,11例住院;相对风险降低50%,95%可信区间3 - 74%,P = 0.06)。符合方案分析显示,15%的远程监测组患者(0例死亡,8例住院)达到主要终点(相对风险降低54%,95%可信区间7 - 79%,P = 0.04)。仅远程监测组患者的纽约心脏协会(NYHA)分级改善了一级(P < 0.001)。在研究期间因心力衰竭恶化住院的远程监测组患者的住院时间明显短于对照组患者(中位6.5天,四分位间距5.5 - 8.3天)(中位10.0天,四分位间距7.0 - 13.0天;P = 0.04)。“从未使用者”的事件发生率不高于对照组患者的事件发生率。
使用移动电话作为患者终端进行远程监测有可能降低心力衰竭住院的频率和持续时间。为老年患者提供用于日常数据采集的合适用户界面仍然是这一概念中具有挑战性的部分。