Queen's University Palliative Care Medicine Program, Kingston, Ontario, Canada.
J Pain Symptom Manage. 2009 Oct;38(4):483-95. doi: 10.1016/j.jpainsymman.2008.12.006. Epub 2009 Aug 21.
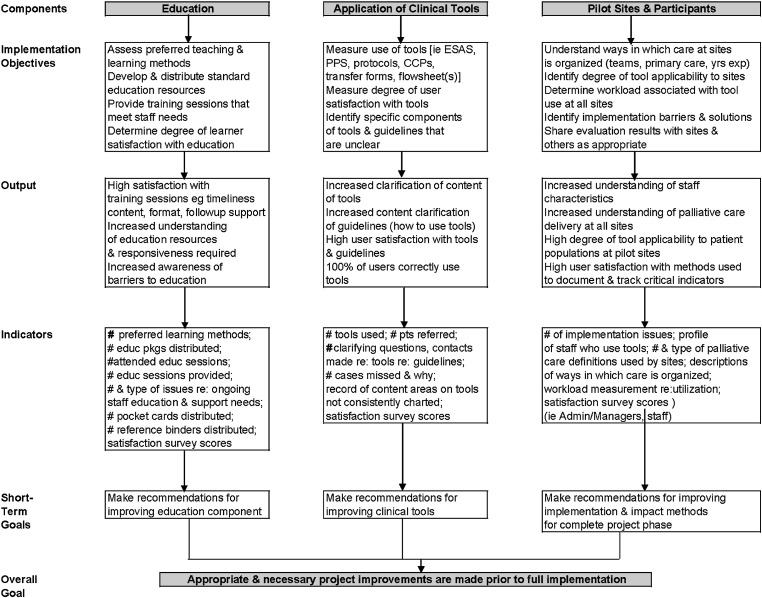
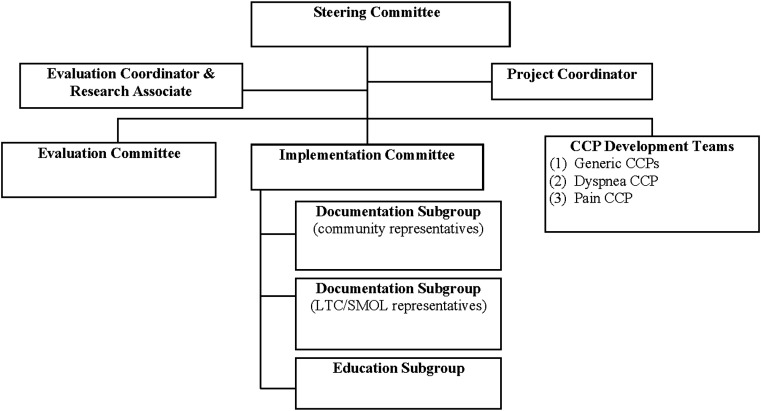
The delivery of optimal palliative care requires an integrated and coordinated approach of many health care providers across the continuum of care. In response to identified gaps in the region, the Palliative Care Integration Project (PCIP) was developed to improve continuity and decrease variability of care to palliative patients with cancer. The infrastructure for the project included multi-institutional and multisectoral representation on the Steering Committee and on the Development, Implementation and Evaluation Working Groups. After review of the literature, five Collaborative Care Plans and Symptom Management Guidelines were developed and integrated with validated assessment tools (Edmonton Symptom Assessment System and Palliative Performance Scale). These project resources were implemented in the community, the palliative care unit, and the cancer center. Surveys were completed by frontline health professionals (defined as health professionals providing direct care), and two independent focus groups were conducted to capture information regarding: 1) the development of the project and 2) the processes of implementation and usefulness of the different components of the project. Over 90 individuals from more than 30 organizations were involved in the development, implementation, and evaluation of the PCIP. Approximately 600 regulated health professionals and allied health professionals who provided direct care, and over 200 family physicians and medical residents, received education/training on the use of the PCIP resources. Despite unanticipated challenges, frontline health professionals reported that the PCIP added value to their practice, particularly in the community sector. The PCIP showed that a network in which each organization had ownership and where no organization lost its autonomy, was an effective way to improve integration and coordination of care delivery.
提供最佳姑息治疗需要许多医疗保健提供者在整个护理连续体中采取综合协调的方法。针对该地区已确定的差距,制定了姑息治疗整合项目(PCIP),以改善对癌症姑息治疗患者的护理连续性并减少护理的变异性。该项目的基础设施包括指导委员会和发展、实施和评估工作组的多机构和多部门代表。在审查文献后,制定了五个协作护理计划和症状管理指南,并与经过验证的评估工具(埃德蒙顿症状评估系统和姑息治疗表现量表)相结合。这些项目资源在社区、姑息治疗病房和癌症中心实施。一线卫生专业人员(定义为提供直接护理的卫生专业人员)完成了调查,并且进行了两个独立的焦点小组,以收集有关以下方面的信息:1)项目的制定,2)项目不同组成部分的实施过程和实用性。来自 30 多个组织的 90 多名人员参与了 PCIP 的制定、实施和评估。大约 600 名提供直接护理的注册卫生专业人员和辅助卫生专业人员以及 200 多名家庭医生和住院医生接受了关于使用 PCIP 资源的教育/培训。尽管面临意外挑战,但一线卫生专业人员报告说,PCIP 为他们的实践增加了价值,特别是在社区部门。PCIP 表明,每个组织都拥有所有权且没有一个组织失去自主权的网络是改善护理提供的整合和协调的有效方法。