Assey Vincent D, Peterson Stefan, Kimboka Sabas, Ngemera Daniel, Mgoba Celestin, Ruhiye Deusdedit M, Ndossi Godwin D, Greiner Ted, Tylleskär Thorkild
Tanzania Food and Nutrition Centre, Dar es Salaam, Tanzania.
BMC Public Health. 2009 Sep 3;9:319. doi: 10.1186/1471-2458-9-319.
In many low-income countries, children are at high risk of iodine deficiency disorders, including brain damage. In the early 1990s, Tanzania, a country that previously suffered from moderate to severe iodine deficiency, adopted universal salt iodation (USI) as an intervention strategy, but its impact remained unknown.
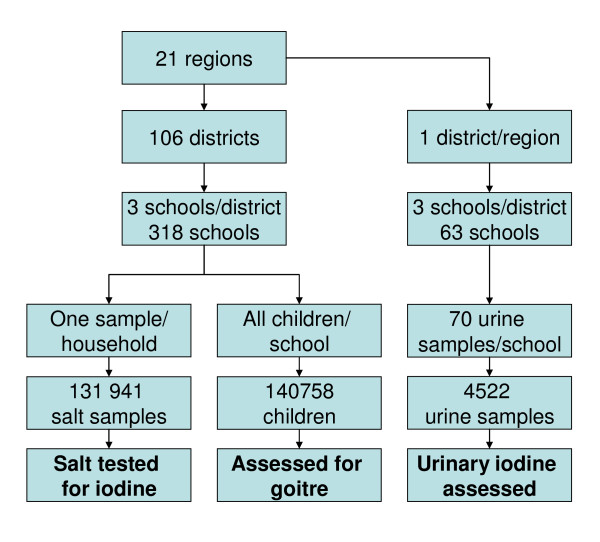
We report on the first national survey in mainland Tanzania, conducted in 2004 to assess the extent to which iodated salt was used and its apparent impact on the total goitre prevalence (TGP) and urinary iodine concentrations (UIC) among the schoolchildren after USI was initiated. In 2004, a cross-sectional goitre survey was conducted; covering 140,758 schoolchildren aged 6 - 18 years were graded for goitre according to new WHO goitre classification system. Comparisons were made with district surveys conducted throughout most of the country during the 1980s and 90s. 131,941 salt samples from households were tested for iodine using rapid field test kits. UIC was determined spectrophotometrically using the ammonium persulfate digestion method in 4523 sub-sampled children.
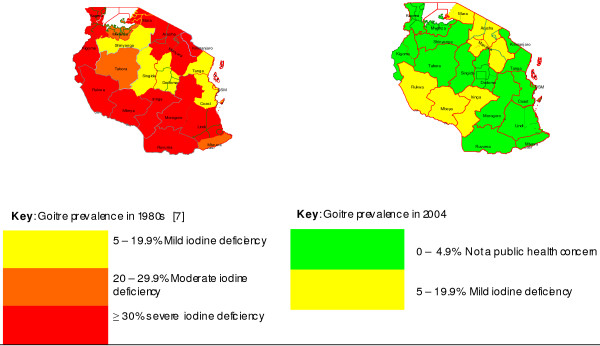
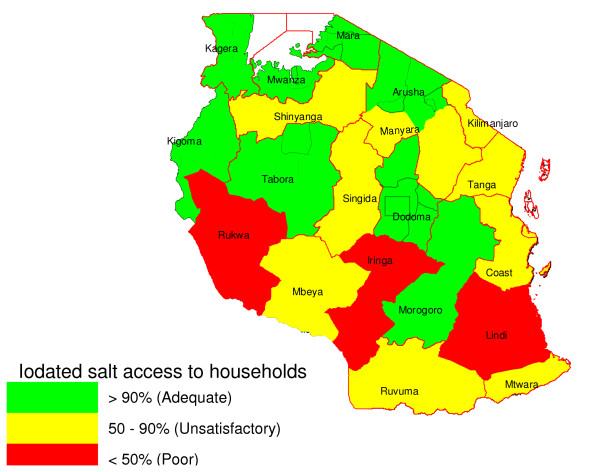
83.6% (95% CI: 83.4 - 83.8) of salt samples tested positive for iodine. Whereas the TGP was about 25% on average in the earlier surveys, it was 6.9% (95%CI: 6.8-7.0) in 2004. The TGP for the younger children, 6-9 years old, was 4.2% (95%CI: 4.0-4.4), n = 41,965. In the 27 goitre-endemic districts, TGP decreased from 61% (1980s) to 12.3% (2004). The median UIC was 204 (95% CF: 192-215) microg/L. Only 25% of children had UIC <100 microg/L and 35% were > or = 300 microg/L, indicating low and excess iodine intake, respectively.
Our study demonstrates a marked improvement in iodine nutrition in Tanzania, twelve years after the initiation of salt iodation programme. The challenge in sustaining IDD elimination in Tanzania is now two-fold: to better reach the areas with low coverage of iodated salt, and to reduce iodine intake in areas where it is excessive. Particular attention is needed in improving quality control at production level and perhaps the national salt iodation regulations may need to be reviewed.
在许多低收入国家,儿童面临碘缺乏疾病的高风险,包括脑损伤。20世纪90年代初,坦桑尼亚这个曾遭受中度至重度碘缺乏的国家,采用了全民食盐碘化(USI)作为干预策略,但其影响仍不明确。
我们报告了2004年在坦桑尼亚大陆进行的首次全国性调查,以评估碘化盐的使用程度及其在启动USI后对学龄儿童甲状腺肿总患病率(TGP)和尿碘浓度(UIC)的明显影响。2004年,进行了一项横断面甲状腺肿调查;根据新的世界卫生组织甲状腺肿分类系统,对140758名6至18岁的学龄儿童进行甲状腺肿分级。与20世纪80年代和90年代在该国大部分地区进行的地区调查进行了比较。使用快速现场检测试剂盒对来自家庭的131941份盐样进行碘检测。在4523名子样本儿童中,采用过硫酸铵消化法通过分光光度法测定UIC。
83.6%(95%可信区间:83.4 - 83.8)的盐样碘检测呈阳性。早期调查中TGP平均约为25%,而2004年为6.9%(95%可信区间:6.8 - 7.0)。6至9岁年幼儿童的TGP为4.2%(95%可信区间:4.0 - 4.4),n = 41965。在27个甲状腺肿流行区,TGP从61%(20世纪80年代)降至12.3%(2004年)。UIC中位数为204(95%可信区间:192 - 215)μg/L。只有25%的儿童UIC<100μg/L,35%的儿童UIC≥300μg/L,分别表明碘摄入量低和过量。
我们的研究表明,在食盐碘化计划启动12年后,坦桑尼亚的碘营养状况有了显著改善。坦桑尼亚在持续消除碘缺乏病方面面临的挑战现在有两个方面:更好地覆盖碘化盐覆盖率低的地区,以及在碘摄入量过高的地区减少碘摄入量。需要特别关注提高生产水平的质量控制,也许国家食盐碘化法规可能需要审查。