Weber Damien C, Wang Hui, Cozzi Luca, Dipasquale Giovanna, Khan Haleem G, Ratib Osman, Rouzaud Michel, Vees Hansjoerg, Zaidi Habib, Miralbell Raymond
Department of Radiation Oncology, University Hospital of Geneva, Geneva, Switzerland.
Radiat Oncol. 2009 Sep 9;4:34. doi: 10.1186/1748-717X-4-34.
A study was performed comparing volumetric modulated arcs (RA) and intensity modulation (with photons, IMRT, or protons, IMPT) radiation therapy (RT) for patients with recurrent prostate cancer after RT.
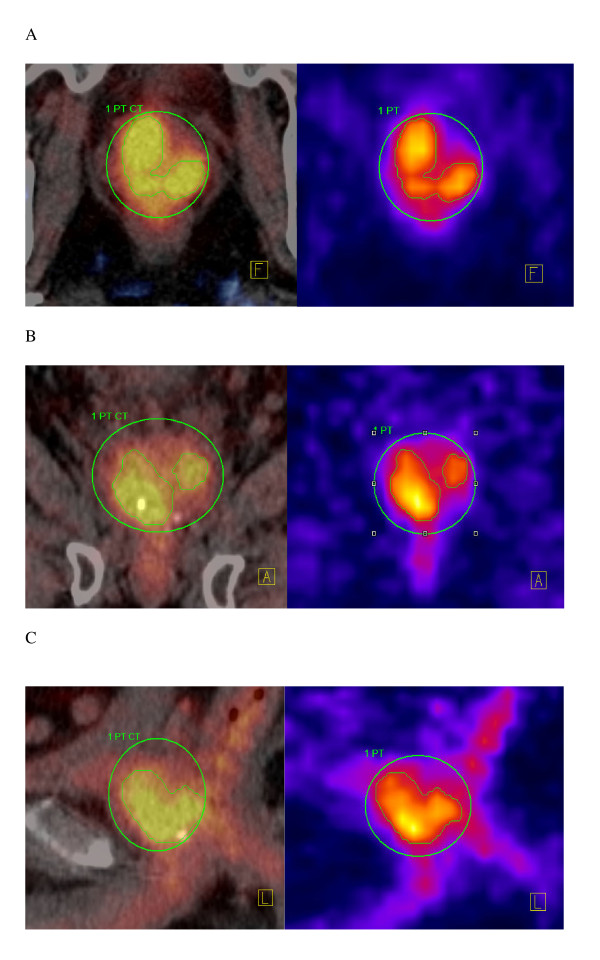
Plans for RA, IMRT and IMPT were optimized for 7 patients. Prescribed dose was 56 Gy in 14 fractions. The recurrent gross tumor volume (GTV) was defined on 18F-fluorocholine PET/CT scans. Plans aimed to cover at least 95% of the planning target volume with a dose > 50.4 Gy. A maximum dose (DMax) of 61.6 Gy was allowed to 5% of the GTV. For the urethra, DMax was constrained to 37 Gy. Rectal DMedian was < 17 Gy. Results were analyzed using Dose-Volume Histogram and conformity index (CI90) parameters.
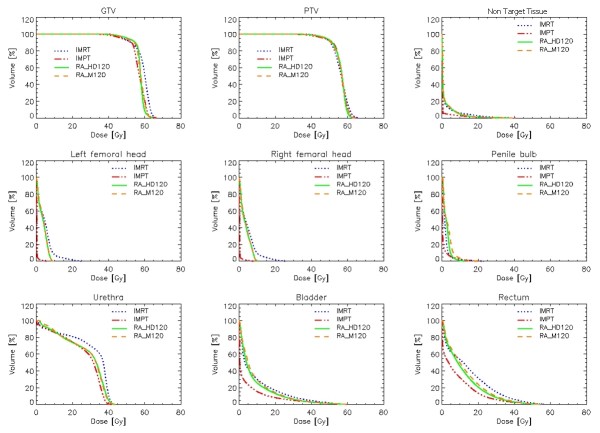
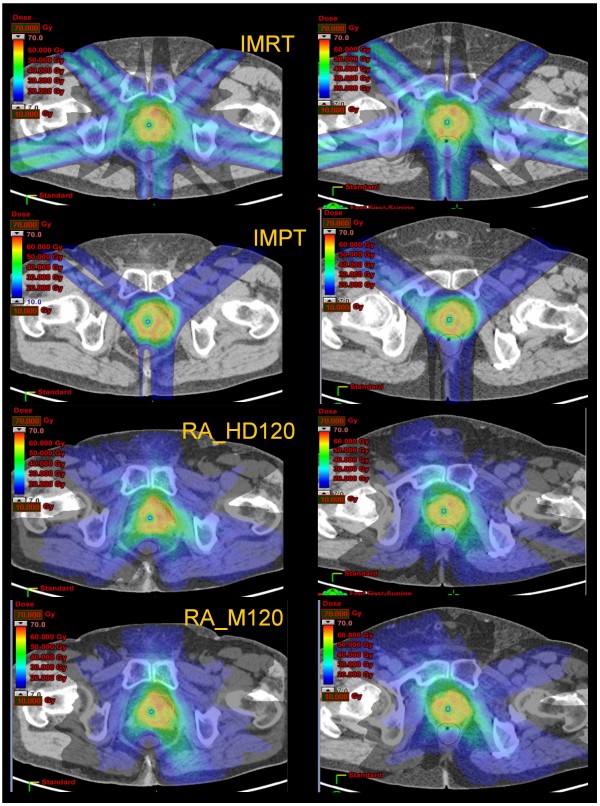
Tumor coverage (GTV and PTV) was improved with RA (V95% 92.6 +/- 7.9 and 83.7 +/- 3.3%), when compared to IMRT (V95% 88.6 +/- 10.8 and 77.2 +/- 2.2%). The corresponding values for IMPT were intermediate for the GTV (V95% 88.9 +/- 10.5%) and better for the PTV (V95%85.6 +/- 5.0%). The percentages of rectal and urethral volumes receiving intermediate doses (35 Gy) were significantly decreased with RA (5.1 +/- 3.0 and 38.0 +/- 25.3%) and IMPT (3.9 +/- 2.7 and 25.1 +/- 21.1%), when compared to IMRT (9.8 +/- 5.3 and 60.7 +/- 41.7%). CI90 was 1.3 +/- 0.1 for photons and 1.6 +/- 0.2 for protons. Integral Dose was 1.1 +/- 0.5 Gy*cm3 *105 for IMPT and about a factor three higher for all photon's techniques.
RA and IMPT showed improvements in conformal avoidance relative to fixed beam IMRT for 7 patients with recurrent prostate cancer. IMPT showed further sparing of organs at risk.
开展了一项研究,比较容积调强弧形放疗(RA)与调强放疗(光子调强放疗,IMRT;或质子调强放疗,IMPT)用于放疗后复发性前列腺癌患者的疗效。
对7例患者的RA、IMRT和IMPT计划进行优化。处方剂量为56 Gy,分14次给予。复发大体肿瘤体积(GTV)通过18F-氟胆碱PET/CT扫描确定。计划旨在使至少95%的计划靶体积接受>50.4 Gy的剂量。允许GTV的5%接受的最大剂量(DMax)为61.6 Gy。对于尿道,DMax限制在37 Gy。直肠中位剂量(DMedian)<17 Gy。使用剂量体积直方图和适形指数(CI90)参数分析结果。
与IMRT(V95%分别为88.6±10.8%和77.2±2.2%)相比,RA的肿瘤覆盖情况(GTV和PTV)有所改善(V95%分别为92.6±7.9%和83.7±3.3%)。IMPT的GTV相应值处于中间水平(V95%为88.9±10.5%),PTV的相应值更好(V95%为85.6±5.0%)。与IMRT(分别为9.8±5.3%和60.7±41.7%)相比,RA(分别为5.1±3.0%和38.0±25.3%)和IMPT(分别为3.9±2.7%和25.1±21.1%)使接受中等剂量(35 Gy)的直肠和尿道体积百分比显著降低。光子放疗的CI90为1.3±0.1,质子放疗的CI90为1.6±0.2。IMPT的积分剂量为1.1±0.5 Gy*cm3 *105,所有光子放疗技术的积分剂量约为其三倍。
对于7例复发性前列腺癌患者,相对于固定束IMRT,RA和IMPT在适形性方面有所改善。IMPT对危及器官的保护作用更强。