Madani Indira, Lomax Antony J, Albertini Francesca, Trnková Petra, Weber Damien C
Center for Proton Therapy, Paul Scherrer Institute, Villigen, Switzerland.
Ghent University, Ghent, Belgium.
Radiat Oncol. 2015 Mar 30;10:72. doi: 10.1186/s13014-015-0384-x.
Newly diagnosed WHO grade II-III or any WHO grade recurrent meningioma exhibit an aggressive behavior and thus are considered as high- or intermediate risk tumors. Given the unsatisfactory rates of disease control and survival after primary or adjuvant radiation therapy, optimization of treatment strategies is needed. We investigated the potential of dose-painting intensity-modulated proton beam-therapy (IMPT) for intermediate- and high-risk meningioma.
Imaging data from five patients undergoing proton beam-therapy were used. The dose-painting target was defined using [68]Ga-[1,4,7,10-tetraazacyclododecane tetraacetic acid]- d-Phe(1),Tyr(3)-octreotate ([68]Ga-DOTATATE)-positron emission tomography (PET) in target delineation. IMPT and photon intensity-modulated radiation therapy (IMRT) treatment plans were generated for each patient using an in-house developed treatment planning system (TPS) supporting spot-scanning technology and a commercial TPS, respectively. Doses of 66 Gy (2.2 Gy/fraction) and 54 Gy (1.8 Gy/fraction) were prescribed to the PET-based planning target volume (PTVPET) and the union of PET- and anatomical imaging-based PTV, respectively, in 30 fractions, using simultaneous integrated boost.
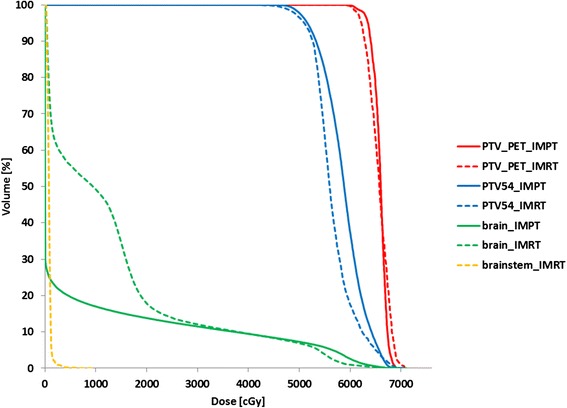
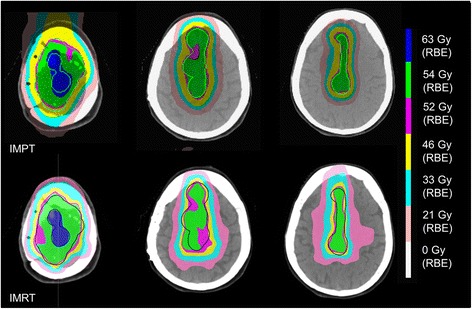
Dose coverage of the PTVsPET was equally good or slightly better in IMPT plans: dose inhomogeneity was 10 ± 3% in the IMPT plans vs. 13 ± 1% in the IMRT plans (p = 0.33). The brain Dmean and brainstem D50 were small in the IMPT plans: 26.5 ± 1.5 Gy(RBE) and 0.002 ± 0.0 Gy(RBE), respectively, vs. 29.5 ± 1.5 Gy (p = 0.001) and 7.5 ± 11.1 Gy (p = 0.02) for the IMRT plans, respectively. The doses delivered to the optic structures were also decreased with IMPT.
Dose-painting IMPT is technically feasible using currently available planning tools and resulted in dose conformity of the dose-painted target comparable to IMRT with a significant reduction of radiation dose delivered to the brain, brainstem and optic apparatus. Dose escalation with IMPT may improve tumor control and decrease radiation-induced toxicity.
新诊断的世界卫生组织(WHO)二级至三级或任何WHO分级的复发性脑膜瘤表现出侵袭性,因此被视为高风险或中风险肿瘤。鉴于原发性或辅助性放射治疗后疾病控制率和生存率不尽人意,需要优化治疗策略。我们研究了剂量调强质子束治疗(IMPT)用于中高危脑膜瘤的潜力。
使用了五名接受质子束治疗患者的影像数据。在靶区勾画中,使用[68]镓-[1,4,7,10-四氮杂环十二烷四乙酸]-d-苯丙氨酸(1),酪氨酸(3)-奥曲肽([68]Ga-DOTATATE)-正电子发射断层扫描(PET)来定义剂量调强靶区。分别使用支持点扫描技术的内部开发治疗计划系统(TPS)和商业TPS为每位患者生成IMPT和光子调强放射治疗(IMRT)治疗计划。采用同步整合加量技术,分别对基于PET的计划靶区(PTVPET)和基于PET与解剖影像的PTV联合靶区给予66 Gy(2.2 Gy/分次)和54 Gy(1.8 Gy/分次)的剂量,分30次给予。
IMPT计划中PTV的剂量覆盖同样良好或略好:IMPT计划中的剂量不均匀性为10±3%,而IMRT计划中为13±1%(p = 0.33)。IMPT计划中脑平均剂量(Dmean)和脑干D50较小:分别为26.5±1.5 Gy(相对生物效应剂量,RBE)和0.002±0.0 Gy(RBE),而IMRT计划中分别为29.5±1.5 Gy(p = 0.001)和7.5±11.1 Gy(p = 0.02)。IMPT还降低了传递至视觉结构的剂量。
使用现有计划工具进行剂量调强IMPT在技术上是可行的,并且剂量调强靶区的剂量适形性与IMRT相当,同时显著降低了传递至脑、脑干和视觉器官的辐射剂量。IMPT剂量递增可能会改善肿瘤控制并降低辐射诱导的毒性。