Toronto Invasive Bacterial Diseases Network, Toronto, Ontario, Canada.
PLoS One. 2009 Sep 29;4(9):e7255. doi: 10.1371/journal.pone.0007255.
Identification of high-risk populations for serious infection due to S. pneumoniae will permit appropriately targeted prevention programs.
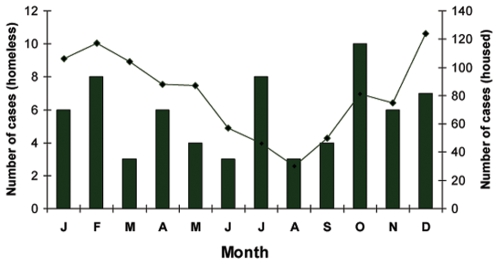
We conducted prospective, population-based surveillance for invasive pneumococcal disease and laboratory confirmed pneumococcal pneumonia in homeless adults in Toronto, a Canadian city with a total population of 2.5 M, from January 1, 2002 to December 31, 2006.
We identified 69 cases of invasive pneumococcal disease and 27 cases of laboratory confirmed pneumococcal pneumonia in an estimated population of 5050 homeless adults. The incidence of invasive pneumococcal disease in homeless adults was 273 infections per 100,000 persons per year, compared to 9 per 100,000 persons per year in the general adult population. Homeless persons with invasive pneumococcal disease were younger than other adults (median age 46 years vs 67 years, P<.001), and more likely than other adults to be smokers (95% vs. 31%, P<.001), to abuse alcohol (62% vs 15%, P<.001), and to use intravenous drugs (42% vs 4%, P<.001). Relative to age matched controls, they were more likely to have underlying lung disease (12/69, 17% vs 17/272, 6%, P = .006), but not more likely to be HIV infected (17/69, 25% vs 58/282, 21%, P = .73). The proportion of patients with recurrent disease was five fold higher for homeless than other adults (7/58, 12% vs. 24/943, 2.5%, P<.001). In homeless adults, 28 (32%) of pneumococcal isolates were of serotypes included in the 7-valent conjugate vaccine, 42 (48%) of serotypes included in the 13-valent conjugate vaccine, and 72 (83%) of serotypes included in the 23-valent polysaccharide vaccine. Although no outbreaks of disease were identified in shelters, there was evidence of clustering of serotypes suggestive of transmission of pathogenic strains within the homeless population.
Homeless persons are at high risk of serious pneumococcal infection. Vaccination, physical structure changes or other program to reduce transmission in shelters, harm reduction programs to reduce rates of smoking, alcohol abuse and infection with bloodborne pathogens, and improved treatment programs for HIV infection may all be effective in reducing the risk.
鉴定因肺炎链球菌引起严重感染的高危人群,将有助于有针对性地开展预防计划。
我们对 2002 年 1 月 1 日至 2006 年 12 月 31 日期间,加拿大多伦多市一个总人口为 250 万的城市中,无家可归的成年人中侵袭性肺炎球菌病和实验室确诊的肺炎球菌性肺炎进行了前瞻性、基于人群的监测。
我们在估计的 5050 名无家可归的成年人中发现了 69 例侵袭性肺炎球菌病和 27 例实验室确诊的肺炎球菌性肺炎。无家可归的成年人侵袭性肺炎球菌病的发病率为每 100000 人每年 273 例感染,而普通成年人的发病率为每 100000 人每年 9 例。患有侵袭性肺炎球菌病的无家可归者比其他成年人年轻(中位数年龄为 46 岁,67 岁,P<.001),并且比其他成年人更有可能吸烟(95%比 31%,P<.001),酗酒(62%比 15%,P<.001),并使用静脉内药物(42%比 4%,P<.001)。与年龄匹配的对照组相比,他们更有可能患有潜在的肺部疾病(12/69,17%比 17/272,6%,P =.006),但并非更容易感染艾滋病毒(17/69,25%比 58/282,21%,P =.73)。无家可归者的复发性疾病比例是其他成年人的五倍(58/58,12%比 24/943,2.5%,P<.001)。在无家可归的成年人中,28 (32%)例肺炎球菌分离株属于 7 价结合疫苗包括的血清型,42 (48%)例属于 13 价结合疫苗包括的血清型,72 (83%)例属于 23 价多糖疫苗包括的血清型。尽管在收容所中没有发现疾病爆发,但有证据表明血清型的聚类表明病原体菌株在无家可归人群中传播。
无家可归者患严重肺炎球菌感染的风险很高。疫苗接种、物理结构改变或其他减少收容所传播的计划、减少吸烟、酗酒和感染血源性病原体的危害减少计划以及改善艾滋病毒感染治疗计划,都可能有助于降低风险。