Wilkowski R, Boeck S, Ostermaier S, Sauer R, Herbst M, Fietkau R, Flentje M, Miethe S, Boettcher H D, Scholten T, Bruns C J, Rau H G, Hinke A, Heinemann V
Department for Radiotherapy and Radiooncology, Klinik Bad Trissl, Oberaudorf, Germany.
Br J Cancer. 2009 Dec 1;101(11):1853-9. doi: 10.1038/sj.bjc.6605420. Epub 2009 Nov 10.
No standard treatment for locally advanced pancreatic cancer (LAPC) is defined.
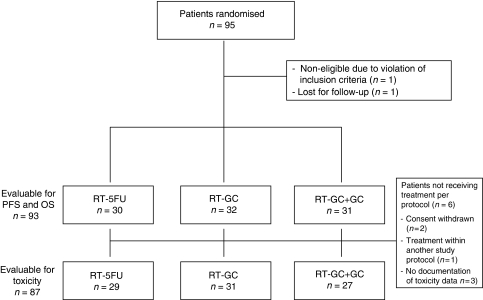
Within a multi-centre, randomised phase II trial, 95 patients with LAPC were assigned to three different chemoradiotherapy (CRT) regimens: patients received conventionally fractionated radiotherapy of 50 Gy and were randomised to concurrent 5-fluorouracil (350 mg m(-2) per day on each day of radiotherapy, RT-5-FU arm), concurrent gemcitabine (300 mg m(-2)), and cisplatin (30 mg m(-2)) on days 1, 8, 22, and 29 (RT-GC arm), or the same concurrent treatment followed by sequential full-dose gemcitabine (1000 mg m(-2)) and cisplatin (50 mg m(-2)) every 2 weeks (RT-GC+GC arm). Primary end point was the overall survival (OS) rate after 9 months.
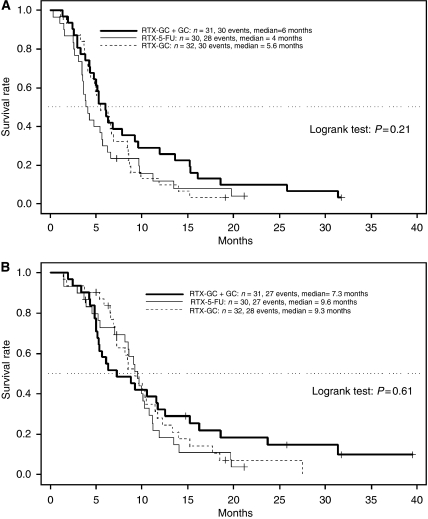
The 9-month OS rate was 58% in the RT-5-FU arm, 52% in the RT-GC arm, and 45% in the RT-GC+GC arm. Corresponding median survival times were 9.6, 9.3, and 7.3 months (P=0.61) respectively. The intent-to-treat response rate was 19, 22, and 13% respectively. Median progression-free survival was estimated with 4.0, 5.6, and 6.0 months (P=0.21). Grade 3/4 haematological toxicities were more frequent in the two GC-containing arms, no grade 3/4 febrile neutropaenia was observed.
None of the three CRT regimens tested met the investigators' definition for efficacy; the median OS was similar to those previously reported with gemcitabine alone in LAPC.
局部晚期胰腺癌(LAPC)尚无标准治疗方案。
在一项多中心随机II期试验中,95例LAPC患者被分配至三种不同的放化疗(CRT)方案:患者接受50 Gy的常规分割放疗,并随机分为三组,分别接受同步5-氟尿嘧啶(放疗期间每日350 mg/m²,RT-5-FU组)、同步吉西他滨(300 mg/m²)和顺铂(第1、8、22和29天30 mg/m²,RT-GC组),或相同的同步治疗后序贯每2周一次的全剂量吉西他滨(1000 mg/m²)和顺铂(50 mg/m²,RT-GC+GC组)。主要终点为9个月后的总生存率(OS)。
RT-5-FU组9个月OS率为58%,RT-GC组为52%,RT-GC+GC组为45%。相应的中位生存时间分别为9.6、9.3和7.3个月(P=0.61)。意向性治疗缓解率分别为19%、22%和13%。中位无进展生存期估计分别为4.0、5.6和6.0个月(P=0.21)。含吉西他滨的两组3/4级血液学毒性更常见,未观察到3/4级发热性中性粒细胞减少。
所测试的三种CRT方案均未达到研究者的疗效定义;中位OS与先前报道的LAPC单纯使用吉西他滨的情况相似。