Department of Health Policy, Planning and Management, Makerere University School of Public Health, P,O, Box 7072, Kampala, Uganda.
Int J Equity Health. 2009 Nov 12;8:39. doi: 10.1186/1475-9276-8-39.
Uganda implemented health sector reforms to make services more accessible to the population. An assessment of the likely impact of these reforms is important for informing policy. This paper describes the changes in utilization of health services that occurred among the poor and those in rural areas between 2002/3 and 2005/6 and associated factors.
Secondary data analysis was done using the socio-economic component of the Uganda National Household Surveys 2002/03 and 2005/06. The poor were identified from wealth quintiles constructed using an asset based index derived from Principal Components Analysis (PCA). The probability of choice of health care provider was assessed using multinomial logistic regression and multi-level statistical models.
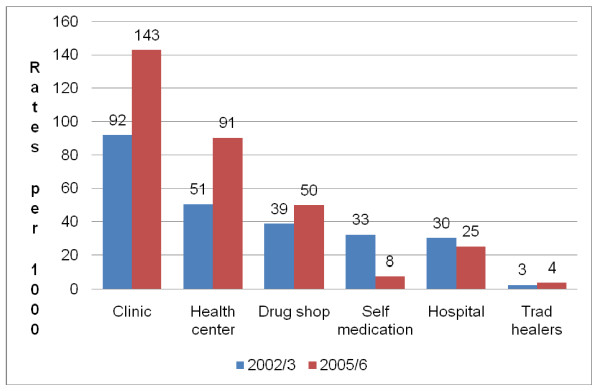
The odds of not seeking care in 2005/6 were 1.79 times higher than in 2002/3 (OR = 1.79; 95% CI 1.65 - 1.94). The rural population experienced a 43% reduction in the risk of not seeking care because of poor geographical access (OR = 0.57; 95% CI 0.48 - 0.67). The risk of not seeking care due to high costs did not change significantly. Private for profit providers (PFP) were the major providers of services in 2002/3 and 2005/6. Using PFP as base category, respondents were more likely to have used private not for profit (PNFP) in 2005/6 than in 2002/3 (OR = 2.15; 95% CI 1.58 - 2.92), and also more likely to use public facilities in 2005/6 than 2002/3 (OR = 1.31; 95% CI 1.15 - 1.48). The most poor, females, rural residents, and those from elderly headed households were more likely to use public facilities relative to PFP.
Although overall utilization of public and PNFP services by rural and poor populations had increased, PFP remained the major source of care. The odds of not seeking care due to distance decreased in rural areas but cost continued to be an important barrier to seeking health services for residents from poor, rural, and elderly headed households. Policy makers should consider targeting subsidies to the poor and rural populations. Public private partnerships should be broadened to increase access to health services among the vulnerable.
乌干达实施了卫生部门改革,以增加民众获得服务的机会。评估这些改革的潜在影响对于为政策提供信息很重要。本文描述了 2002/3 年至 2005/6 年间,贫困人群和农村地区的卫生服务利用情况发生的变化,以及相关因素。
利用 2002/03 年和 2005/06 年乌干达国家住户调查的社会经济部分进行二次数据分析。使用基于主成分分析(PCA)得出的资产指数构建的财富五分位数来确定贫困人口。使用多项逻辑回归和多层次统计模型评估选择医疗服务提供者的概率。
2005/6 年不寻求医疗服务的可能性比 2002/3 年高 1.79 倍(OR=1.79;95%CI 1.65-1.94)。农村地区由于地理位置不便而不寻求医疗服务的风险降低了 43%(OR=0.57;95%CI 0.48-0.67)。由于费用高而不寻求医疗服务的风险没有显著变化。私营营利性提供者(PFP)是 2002/3 年和 2005/6 年的主要服务提供者。以 PFP 为基础类别,与 2002/3 年相比,受访者在 2005/6 年更有可能使用私营非营利性提供者(PNFP)(OR=2.15;95%CI 1.58-2.92),也更有可能在 2005/6 年使用公共设施(OR=1.31;95%CI 1.15-1.48)。最贫困、女性、农村居民和老年人家庭的人更有可能使用公共设施,而不是 PFP。
尽管农村和贫困人口对公共和 PNFP 服务的总体利用率有所增加,但 PFP 仍然是主要的服务来源。由于距离而不寻求医疗服务的可能性在农村地区有所下降,但费用仍然是贫困、农村和老年人家庭居民寻求医疗服务的一个重要障碍。政策制定者应考虑向贫困人口和农村人口提供补贴。应扩大公私伙伴关系,以增加弱势群体获得卫生服务的机会。