The Ohio State University, Columbus, OH 43074, USA.
Curr Med Res Opin. 2010 Jan;26(1):129-37. doi: 10.1185/03007990903437412.
To evaluate symptom control and tolerability after abrupt conversion from oral extended-release methylphenidate (ER-MPH) to methylphenidate transdermal system (MTS) via a dose-transition schedule in children with attention-deficit/hyperactivity disorder (ADHD).
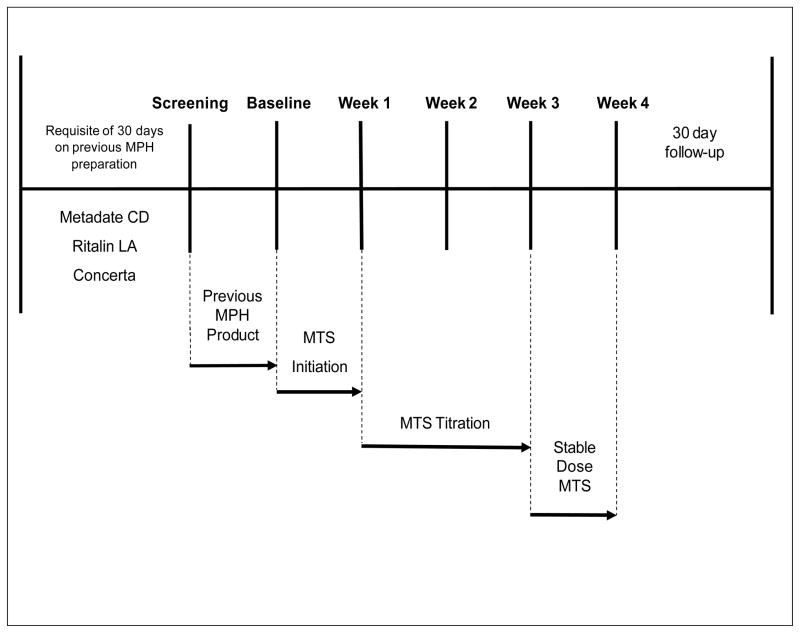
In a 4-week, prospective, multisite, open-label study, 171 children (164 intent-to-treat) with diagnosed ADHD aged 6-12 years abruptly switched from a stable dose of oral ER-MPH to MTS in nominal dosages of 10, 15, 20, and 30 mg using a predefined dose-transition schedule. After the first week on the scheduled dose, the dose was titrated to optimal effect. The primary effectiveness outcome was the change from baseline (while taking ER-MPH) to week 4 in ADHD-Rating Scale-IV (ADHD-RS-IV) total scores. Adverse events (AEs) were assessed throughout the study.
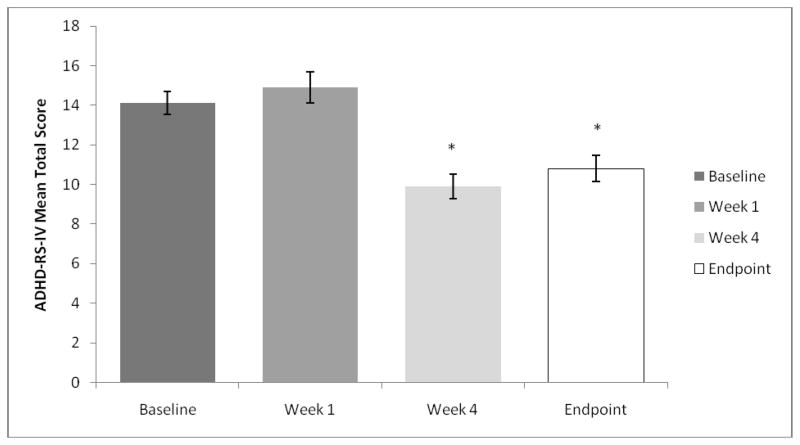
Most subjects (58%) remained on the initial MTS dose defined by the dose-transition schedule; 38% increased and 4% decreased their MTS dose for optimization. MTS dose optimization resulted in significantly better ADHD-RS-IV total (mean +/- SD) scores at week 4 than at baseline (9.9 +/- 7.47 vs. 14.1 +/- 7.48; p < 0.0001). The most commonly reported AEs included headache, decreased appetite, insomnia, and upper abdominal pain. Four subjects (2.3%) discontinued because of application site reactions and three discontinued because of other AEs.
Abrupt conversion from a stable dose of oral ER-MPH to MTS was accomplished using a predefined dose-transition schedule without loss of symptom control; however, careful titration to optimal dose is recommended. Most AEs were mild to moderate and, with the exception of application site reactions, were similar to AEs typically observed with oral MPH. Limitations of this study included its open-label sequential design without placebo, which could result in spurious attribution of improvement to the study treatment and precluded superiority determinations of MTS over baseline ER-MPH treatment. The apparent superiority of MTS was likely due to more careful titration and clinical monitoring rather than the product itself. ClinicalTrials.gov: NCT00151983.
评估通过剂量转换方案从口服缓释哌醋甲酯(ER-MPH)转换为哌醋甲酯透皮系统(MTS)后,患有注意缺陷多动障碍(ADHD)的儿童的症状控制和耐受性。
在一项为期 4 周、前瞻性、多中心、开放标签的研究中,171 名年龄在 6-12 岁、被诊断患有 ADHD 的儿童(164 名意向治疗)以既定剂量从稳定剂量的口服 ER-MPH 转换为 MTS,使用预设的剂量转换方案,名义剂量为 10、15、20 和 30mg。在接受预定剂量的第一周后,根据最佳疗效调整剂量。主要疗效结局是从基线(服用 ER-MPH 时)到第 4 周时 ADHD 评定量表-IV(ADHD-RS-IV)总分的变化。整个研究期间评估不良事件(AE)。
大多数受试者(58%)按剂量转换方案规定的初始 MTS 剂量维持治疗;38%增加剂量,4%减少剂量以优化疗效。MTS 剂量优化使第 4 周的 ADHD-RS-IV 总分(均值±SD)明显优于基线(9.9±7.47 与 14.1±7.48;p<0.0001)。最常报告的 AE 包括头痛、食欲减退、失眠和上腹痛。4 名受试者(2.3%)因用药部位反应而停药,3 名因其他 AE 而停药。
使用预设的剂量转换方案从口服 ER-MPH 的稳定剂量转换为 MTS 而不丧失症状控制;然而,建议仔细滴定至最佳剂量。大多数 AE 为轻度至中度,除用药部位反应外,与口服 MPH 通常观察到的 AE 相似。本研究的局限性包括其开放性、顺序设计而无安慰剂,这可能导致改善归因于研究治疗而产生虚假效应,并排除 MTS 相对于基线 ER-MPH 治疗的优越性。MTS 的明显优越性可能是由于更仔细的滴定和临床监测,而不是产品本身。ClinicalTrials.gov:NCT00151983。