Silvestre Joana, Santos Luis, Batalha Vitor, Del Rio Ana, Lima Carlos, Carvalho Antonio, Martins Ana, Miranda Helena, Cabral Fatima, Felix Adelia, Aleixo Ana
Medicine IV Department, São Francisco Xavier Hospital, Estrada do Forte do Alto do Duque, 1449-005 Lisbon, Portugal.
J Med Case Rep. 2009 Nov 2;3:95. doi: 10.1186/1752-1947-3-95.
Paraneoplastic necrotizing myopathy is a rare disorder, described as a proximal, symmetrical, and rapidly progressing myopathy that is manifested as a paraneoplastic syndrome. Diagnosis is established via histological examination of the muscle biopsy.
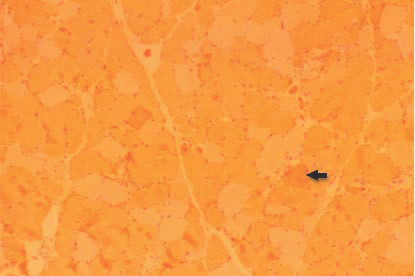
We present the case of a 53-year-old woman, born in Guinea-Bissau, with a history of locally advanced breast cancer, diagnosed ten months previously. The patient had experienced a progressively proximal muscle weakness of the lower extremities, which led to a total inability to walk. Upon neurological examination, the patient showed muscle weakness and atrophy in both proximal lower extremities without myalgia. Muscle strength was graded according to the Medical Research Council Scale as 2 out of 5 in the bilateral iliopsoas muscle, and 4 out of 5 in the bilateral quadriceps femoris. The deep-tendon reflexes were hypoactive. The laboratory examination showed increased values of serum creatinine kinase and myoglobin. An electromyogram showed an incomplete interference pattern during voluntary contraction in the iliopsoas and quadriceps femoris. The motor nerve conduction was 44.1 m/s and 44.3 m/s in the right and left tibial nerves, respectively, and 46.5 m/s and 46.1 m/s in the right and left peroneal nerves, respectively. The sensory motor nerve conductions and the compound motor action potential amplitudes were normal. These findings, despite not being specific, suggested a myopathy. Consequently, a muscle biopsy was performed. A biopsy specimen showed myopathic changes that were characteristic of a necrotizing myopathy.
Treatment for this syndrome consists of controlling the tumor, and providing corticoid therapy. This led to the partial remission of the neurological manifestations.
副肿瘤性坏死性肌病是一种罕见的疾病,被描述为一种近端、对称性且进展迅速的肌病,表现为副肿瘤综合征。通过肌肉活检的组织学检查来确诊。
我们报告一例53岁女性病例,她出生于几内亚比绍,有局部晚期乳腺癌病史,于10个月前确诊。患者出现了下肢近端肌肉无力逐渐加重,最终完全无法行走。经神经学检查,患者双下肢近端肌肉无力且萎缩,无肌痛。根据医学研究委员会量表,双侧髂腰肌肌力分级为2级(满分5级),双侧股四头肌肌力分级为4级(满分5级)。深腱反射减弱。实验室检查显示血清肌酐激酶和肌红蛋白值升高。肌电图显示髂腰肌和股四头肌在自主收缩时呈不完全干扰型。右侧和左侧胫神经运动神经传导速度分别为44.1米/秒和44.3米/秒,右侧和左侧腓总神经运动神经传导速度分别为46.5米/秒和46.1米/秒。感觉运动神经传导和复合运动动作电位幅度正常。这些发现虽然不具有特异性,但提示为肌病。因此,进行了肌肉活检。活检标本显示出坏死性肌病的特征性肌病改变。
该综合征的治疗包括控制肿瘤和给予皮质类固醇治疗。这导致神经学表现部分缓解。