Rowley Scott M
The Ohio State University Comprehensive Cancer Center - Arthur G. James Cancer Hospital and Richard J. Solove Research Institute.
J Adv Pract Oncol. 2018 Mar;9(2):216-221. Epub 2018 Mar 1.
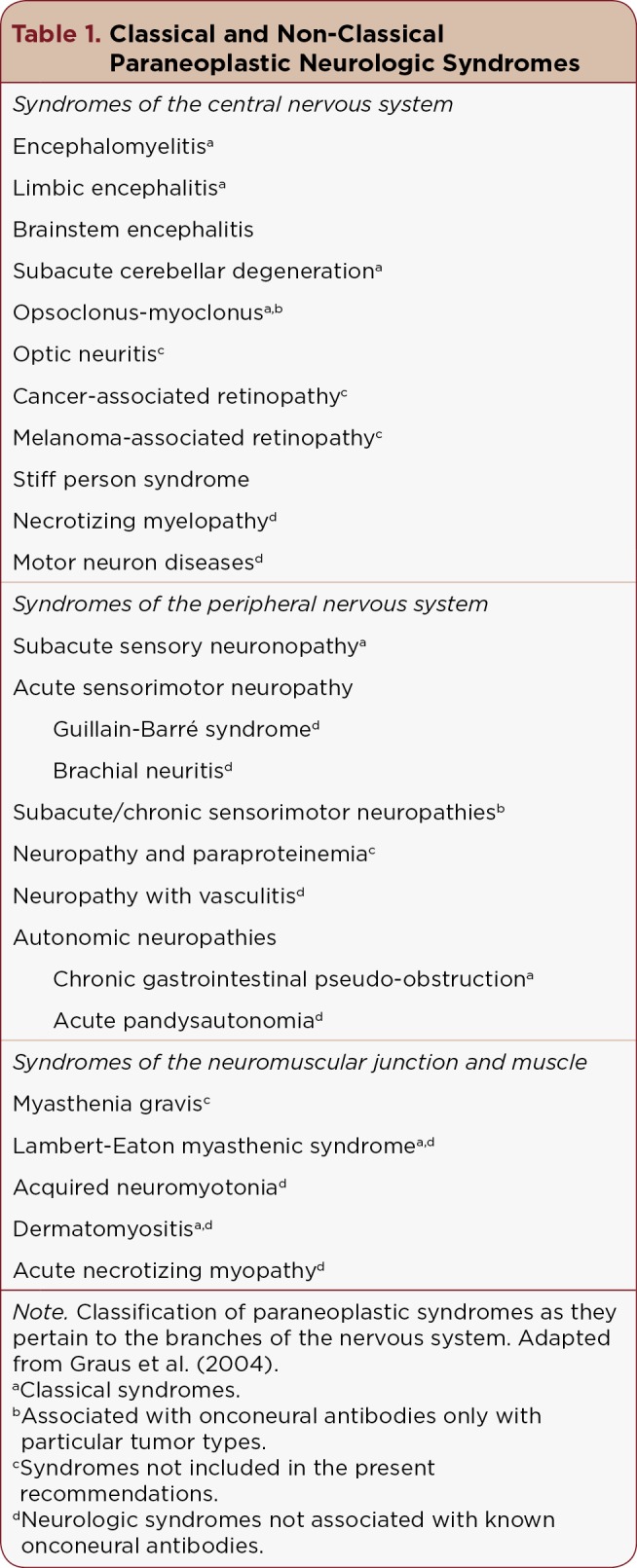
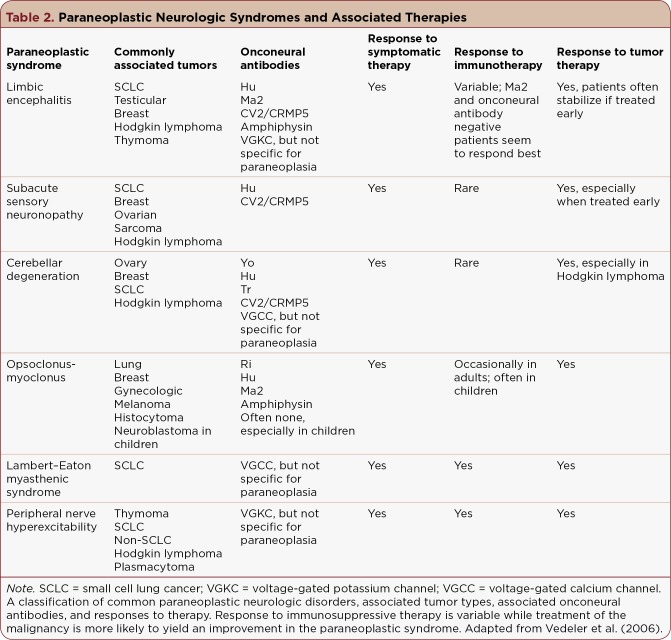
RS, a 36-year-old female, presented to the emergency department (ED) of a large academic medical center upon the advice of her primary care provider because of 3 weeks of progressive mental status changes, weakness, and decreased oral intake. According to her husband, RS was diagnosed with stage IIIA large cell lung cancer 8 months earlier and was treated with concurrent chemotherapy (carboplatin, pemetrexed, and bevacizumab) and radiation therapy that was completed 4 months prior to admission. No other specific information about her treatment or outside health records was available. According to her husband, RS had been in her usual state of health until approximately 3 weeks prior, when she began having significant mental status changes. She first exhibited some difficulty finding words and later was noted to be putting food in a coffee maker. This spontaneously resolved after approximately 1 week; however, she rapidly developed slurred speech and began to make nonsensical statements. These manifestations also slowly improved but were followed by worsening speech deficit, difficulty walking, and impaired balance. During one of these episodes, she had an occurrence of incontinence. Her husband also noted an incident where her "eyes were beating back and forth and the left side of her face was twitching." RS also had periods (according to her husband) where she "did not seem to be interacting with her environment." These progressively worsened during the last week, and she completely stopped walking and talking 2 days prior to coming to the ED. According to her husband, RS had rheumatoid arthritis and no surgical history. Her family history was unknown except that RS's mother had "seizures." RS had reportedly not used tobacco, alcohol, or drugs, and she was sexually active with her husband. Home medications included transdermal fentanyl 12 μg/hr patch changed every 72 hours; oxycodone-acetaminophen tablets 5-325 mg, two every 4 hours as needed for pain; prednisone 10 mg, one tablet daily; and megestrol 40 mg/mL suspension, 20 mL once daily for appetite stimulation. RS was admitted to an inpatient medical oncology service and evaluated by the oncology advanced practitioner (AP) on her second inpatient day. Upon exam, RS was nonverbal except for moaning in response to painful stimuli and to her sister's voice. Her vital signs were normal. She appeared ill but well-nourished, and she was mildly diaphoretic. Neurologic examination revealed that her pupils were slightly sluggish but equal, round, and reactive to light. Extraocular muscle movements were intact, but she did not move her eyes in response to commands. She tracked the AP and family members around the room with her eyes. Cranial nerve examination was intact with the exception of cranial nerves IX, X, and XI, which were difficult to examine given her inability to cooperate and open her mouth. Motor examination revealed increased tone throughout and intermittent, inconsistent resistance to passive movement. She was seen to move all four extremities spontaneously although not in response to commands. Deep tendon reflexes were intact and equal in all extremities. Examination of other body systems was as follows: there was dry, peeling skin on her lips, but her mucous membranes were moist and free of erythema or lesions. Her lungs were clear to auscultation bilaterally. Her heart rate and rhythm were regular, there were no murmurs, rubs, or gallops, and distal pulses were intact. Her abdomen was nondistended with normally active bowel sounds in all four quadrants. Her abdomen was soft, nontender to palpation, and without palpable masses. There was no peripheral discoloration, temperature changes, or edema, and examination of her skin was benign. On admission to the emergency department, serum laboratory studies were unrevealing for any potential causes of encephalopathy. Kidney and liver function were normal, making diagnoses of uremic and hepatic encephalopathies less likely. Cultures of the urine and blood were negative. Samples of cerebrospinal fluid (CSF) were obtained via lumbar puncture and were unrevealing for any abnormalities. Computed tomography (CT) of the head without contrast was negative for any acute intracranial process. Ultrasound of the right upper quadrant revealed a single, nonspecific, hypoechoic hepatic lesion. Computed tomography scans of the chest, abdomen, and pelvis demonstrated the primary malignancy in the upper lobe of the left lung, as well as possible metastatic disease within the left lung, right lung, and liver, and widespread osseous metastatic disease. Magnetic resonance imaging (MRI) of the brain performed 1 day after admission demonstrated numerous scattered punctate foci of enhancement throughout the supratentorial and infratentorial brain parenchyma, measuring at most 3 to 4 millimeters in diameter. There was no significant mass effect or midline shift. A paraneoplastic panel was sent to an outside laboratory and returned positive for antivoltage-gated potassium channel (VGKC) autoantibodies. Clinically, RS was exhibiting signs of encephalopathy, a broad term that indicates general brain dysfunction, the hallmark of which is altered mental status. Diagnosing encephalopathy is challenging, as many differential diagnoses must be considered. The clinician must consider metabolic derangements, toxic and infectious etiologies, psychiatric disorders, and less commonly, prion disorders and progressive dementia. Cultures of RS's blood and urine as well as other specialized endocrine tests were negative, decreasing the likelihood of a metabolic or infectious cause for her presentation. The abnormalities on her brain MRI were reviewed by a neuro-oncology team, who felt that the faint, nondescript nature of the visualized lesions was not suspicious for metastatic disease. Sequelae of seizures was also considered by neuro-oncology but dismissed given a grossly normal prolonged electroencephalogram. Some encephalopathies are caused by autoimmune or inflammatory mechanisms, which are confirmed by the presence of autoantibody markers and/or clear response to immunomodulatory treatment (Vernino, Geschwind, & Boeve, 2007). These types of encephalopathies have been seen in patients with cancer and have thus been termed paraneoplastic. The presence of anti-VGKC antibodies on RS's paraneoplastic panel directed the inpatient medical oncology team toward a paraneoplastic neurologic disorder (PND) as the most likely diagnosis.
RS是一名36岁女性,在其初级保健医生的建议下,前往一家大型学术医疗中心的急诊科就诊,原因是持续3周的精神状态改变、虚弱和口腔摄入量减少。据她丈夫称,RS在8个月前被诊断为IIIA期大细胞肺癌,并接受了同步化疗(卡铂、培美曲塞和贝伐单抗)和放射治疗,放疗在入院前4个月完成。没有关于她的治疗或外部健康记录的其他具体信息。据她丈夫说,RS一直处于平常的健康状态,直到大约3周前,她开始出现明显的精神状态改变。她首先表现出一些找词困难,后来被发现把食物放进咖啡机里。这种情况在大约1周后自行缓解;然而,她迅速出现言语不清,并开始说一些无意义的话。这些表现也逐渐改善,但随后出现言语缺陷加重、行走困难和平衡受损。在其中一次发作期间,她出现了失禁。她丈夫还提到有一次她“眼睛来回跳动,左脸抽搐”。RS也有一段时间(据她丈夫说)“似乎没有与周围环境互动”。在最后一周,这些情况逐渐恶化,在前往急诊科的前两天,她完全停止了行走和说话。据她丈夫说,RS患有类风湿性关节炎,没有手术史。除了RS的母亲有“癫痫发作”外,她的家族病史不详。据报道,RS不吸烟、不饮酒、不吸毒,并且与丈夫有性生活。家庭用药包括每72小时更换一次的12μg/小时透皮芬太尼贴剂;5-325mg羟考酮-对乙酰氨基酚片,必要时每4小时两片用于止痛;泼尼松10mg,每日一片;以及40mg/mL甲地孕酮混悬液,每日20mL用于刺激食欲。RS被收治到住院医疗肿瘤服务部门,并在住院第二天由肿瘤学高级执业医师(AP)进行评估。检查时,RS除了对疼痛刺激和她姐姐的声音发出呻吟外,无法言语。她的生命体征正常。她看起来病恹恹的,但营养良好,并且有轻微出汗。神经系统检查显示她的瞳孔略迟缓,但等大、圆形,对光有反应。眼外肌运动正常,但她不根据指令移动眼睛。她用眼睛追踪房间里的AP和家庭成员。除了第九、第十和第十一对颅神经外,颅神经检查正常,由于她无法配合和张嘴,这几对颅神经难以检查。运动检查显示全身肌张力增加,对被动运动有间歇性、不一致的抵抗。可以看到她四肢自发移动,尽管不是对指令的反应。四肢的深腱反射正常且对称。其他身体系统的检查如下:她的嘴唇有干燥、脱皮的皮肤,但黏膜湿润,没有红斑或病变。双侧肺部听诊清晰。她的心率和节律正常,没有杂音、摩擦音或奔马律,远端脉搏正常。她的腹部无膨隆,四个象限的肠鸣音正常活跃。她的腹部柔软,触诊无压痛,没有可触及的肿块。没有外周变色、温度变化或水肿,皮肤检查正常。在急诊科入院时,血清实验室检查未发现任何可能导致脑病的原因。肾功能和肝功能正常,因此不太可能诊断为尿毒症和肝性脑病。尿液和血液培养均为阴性。通过腰椎穿刺获取脑脊液(CSF)样本,未发现任何异常。头颅无对比剂计算机断层扫描(CT)未发现任何急性颅内病变。右上腹超声显示一个单一的、非特异性的、低回声肝脏病变。胸部、腹部和骨盆的计算机断层扫描显示左肺上叶有原发性恶性肿瘤,以及左肺、右肺和肝脏内可能的转移性疾病,以及广泛的骨转移性疾病。入院后1天进行的脑部磁共振成像(MRI)显示,幕上和幕下脑实质内有许多散在的点状强化灶,直径最大为3至4毫米。没有明显的占位效应或中线移位。一个副肿瘤检测 panel 被送往外部实验室,结果显示抗电压门控钾通道(VGKC)自身抗体呈阳性。临床上,RS表现出脑病的症状,脑病是一个广义的术语,表明一般的脑功能障碍,其标志是精神状态改变。诊断脑病具有挑战性,因为必须考虑许多鉴别诊断。临床医生必须考虑代谢紊乱、中毒和感染性病因、精神疾病,以及较少见的朊病毒疾病和进行性痴呆。RS的血液和尿液培养以及其他专门的内分泌检查均为阴性,降低了她出现代谢或感染性病因的可能性。神经肿瘤学团队对她脑部MRI的异常情况进行了复查,他们认为所观察到的病变微弱、不明确的性质不怀疑是转移性疾病。神经肿瘤学也考虑了癫痫发作的后遗症,但由于脑电图长时间大致正常而排除了这种可能性。一些脑病是由自身免疫或炎症机制引起的,这通过自身抗体标志物的存在和/或对免疫调节治疗的明确反应得到证实(Vernino、Geschwind和Boeve,2007年)。这些类型的脑病在癌症患者中可见,因此被称为副肿瘤性。RS的副肿瘤检测 panel 上抗VGKC抗体的存在使住院医疗肿瘤学团队将副肿瘤性神经系统疾病(PND)作为最可能的诊断。