Emergency Department, Kaiser Permanente San Rafael, San Rafael, CA 94903, USA.
Med Care. 2010 Jan;48(1):58-63. doi: 10.1097/MLR.0b013e3181bd49ad.
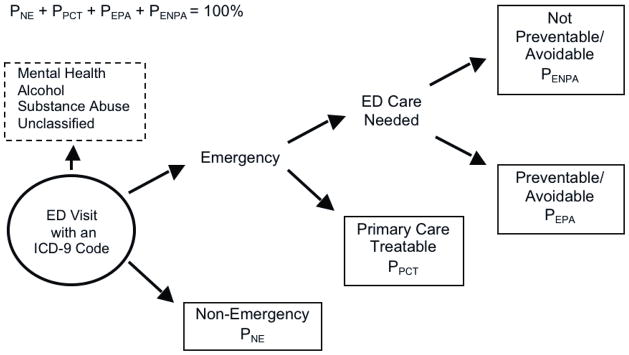
Differentiating between appropriate and inappropriate resource use represents a critical challenge in health services research. The New York University Emergency Department (NYU ED) visit severity algorithm attempts to classify visits to the ED based on diagnosis, but it has not been formally validated.
To assess the validity of the NYU algorithm.
A longitudinal study in a single integrated delivery system from January 1999 to December 2001.
A total of 2,257,445 commercial and 261,091 Medicare members of an integrated delivery system.
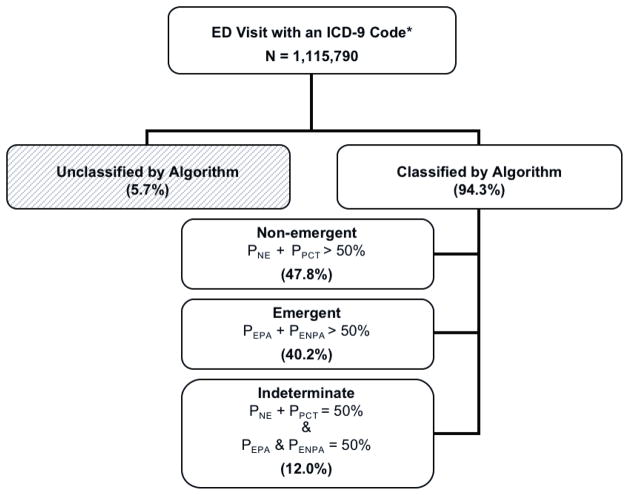
ED visits were classified as emergent, nonemergent, or intermediate severity, using the NYU ED algorithm. We examined the relationship between visit-severity and the probability of future hospitalizations and death using a logistic model with a general estimating equation approach.
Among commercially insured subjects, ED visits categorized as emergent were significantly more likely to result in a hospitalization within 1-day (odds ratio = 3.37, 95% CI: 3.31-3.44) or death within 30-days (odds ratio = 2.81, 95% CI: 2.62-3.00) than visits categorized as nonemergent. We found similar results in Medicare patients and in sensitivity analyses using different probability thresholds. ED overuse for nonemergent conditions was not related to socio-economic status or insurance type.
The evidence presented supports the validity of the NYU ED visit severity algorithm for differentiating ED visits based on need for hospitalization and/or mortality risk; therefore, it can contribute to evidence-based policies aimed at reducing the use of the ED for nonemergencies.
区分适当和不适当的资源利用是卫生服务研究中的一个关键挑战。纽约大学急诊部(NYU ED)就诊严重程度算法试图根据诊断对 ED 就诊进行分类,但尚未经过正式验证。
评估 NYU 算法的有效性。
一项单中心一体化交付系统的纵向研究,时间为 1999 年 1 月至 2001 年 12 月。
一个一体化交付系统的商业保险和医疗保险共 2,257,445 名成员和 261,091 名成员。
使用 NYU ED 算法将 ED 就诊分为紧急、非紧急或中度严重程度。我们使用具有广义估计方程方法的逻辑模型检查就诊严重程度与未来住院和死亡的概率之间的关系。
在商业保险患者中,被归类为紧急的 ED 就诊在 1 天内住院的可能性明显更高(优势比=3.37,95%置信区间:3.31-3.44)或在 30 天内死亡的可能性更高(优势比=2.81,95%置信区间:2.62-3.00),而非紧急就诊。我们在 Medicare 患者中发现了类似的结果,并且在使用不同概率阈值的敏感性分析中也得到了类似的结果。对于非紧急情况,ED 过度使用与社会经济地位或保险类型无关。
所提供的证据支持 NYU ED 就诊严重程度算法区分基于住院和/或死亡率风险的 ED 就诊的有效性;因此,它可以为旨在减少 ED 对非紧急情况使用的基于证据的政策做出贡献。