Department of Emergency Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2018 Oct 5;1(6):e183731. doi: 10.1001/jamanetworkopen.2018.3731.
Insurers have increasingly adopted policies to reduce emergency department (ED) visits that they consider unnecessary. One common approach is to retrospectively deny coverage if the ED discharge diagnosis is determined by the insurer to be nonemergent.
To characterize ED visits that may be denied coverage if the ED coverage denial policy of a large national insurer, Anthem, Inc, is widely adopted.
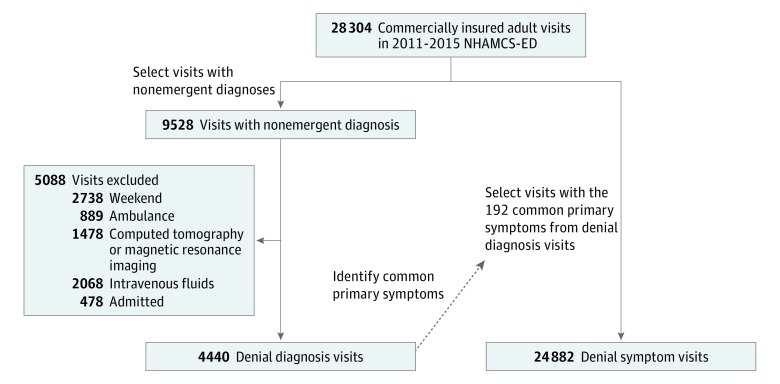
DESIGN, SETTING, AND PARTICIPANTS: A cross-sectional analysis of probability-sampled ED visits from the nationally representative National Hospital Ambulatory Medical Care Survey ED subsample occurring from January 1, 2011, to December 31, 2015, was conducted. Visits by commercially insured patients aged 15 to 64 years were examined. Those with ED discharge diagnoses defined by Anthem's policy as nonemergent and therefore subject to possible denial of coverage were classified as denial diagnosis visits. The primary presenting symptoms among denial diagnosis visits were identified, and all visits by commercially insured adults presenting with these primary symptoms were classified as denial symptom visits.
Each visit cohort as a weighted proportion of commercially insured adult ED visits. The proportion of each visit cohort that received ED-level care, defined as visits where patients were triaged as urgent or emergent, received 2 or more diagnostic tests, or were admitted or transferred, was also examined.
From 2011 to 2015, 15.7% (95% CI, 15.0%-16.4%) of commercially insured adult ED visits (4440 of 28 304) were denial diagnosis visits (mean [SD] patient age, 36.6 [14.0] years; 2592 [58.7%] female and 2962 [63.5%] white). Among these visits, 39.7% (95% CI, 37.1%-42.3%) received ED-level care: 24.5% (95% CI, 21.7%-27.4%) were initially triaged as urgent or emergent and 26.0% (95% CI, 23.8%-28.3%) received 2 or more diagnostic tests. These denial diagnosis visits shared the same presenting symptoms as 87.9% (95% CI, 87.3%-88.4%) of commercially insured adult ED visits (24 882 of 28 304) (mean [SD] patient age, 38.5 [14.1] years; 14 362 [57.9%] female and 17 483 [68.7%] white). Among these denial symptom visits, 65.1% (95% CI, 63.4%-66.9%) received ED-level care: 43.2% (95% CI, 40.2%-46.4%) were triaged as urgent or emergent, 51.9% (95% CI, 50.0%-53.9%) received 2 or more diagnostic tests, and 9.7% (95% CI, 8.8%-10.6%) were admitted or transferred.
Anthem's nonemergent ED discharge diagnoses were not associated with identification of unnecessary ED visits when assessed from the patient's perspective. This cost-reduction policy could place many patients who reasonably seek ED care at risk of coverage denial.
保险公司越来越多地采取政策来减少他们认为不必要的急诊(ED)就诊。一种常见的方法是,如果保险公司确定 ED 出院诊断为非紧急情况,就追溯性地拒绝承保。
描述如果大型全国保险公司 Anthem,Inc. 的 ED 承保拒绝政策被广泛采用,可能会被拒绝承保的 ED 就诊。
设计、地点和参与者:对 2011 年 1 月 1 日至 2015 年 12 月 31 日期间全国代表性的国家医院门诊医疗调查 ED 子样本中的概率抽样 ED 就诊进行了横断面分析。研究对象为年龄在 15 至 64 岁之间的商业保险患者。将 ED 出院诊断被 Anthem 的政策定义为非紧急且因此可能被拒绝承保的就诊归类为拒绝诊断就诊。确定了拒绝诊断就诊中的主要就诊症状,并将所有商业保险成人以这些主要症状就诊的就诊归类为拒绝症状就诊。
每个就诊队列作为商业保险成人 ED 就诊的加权比例。还检查了每个就诊队列中接受 ED 级护理的比例,定义为患者被分诊为紧急或紧急、接受 2 项或更多诊断性检查或住院或转院的就诊比例。
2011 年至 2015 年,商业保险成年 ED 就诊中有 15.7%(95%CI,15.0%-16.4%)(28304 例就诊中的 4440 例)为拒绝诊断就诊(平均[SD]患者年龄为 36.6[14.0]岁;2592[58.7%]为女性,2962[63.5%]为白人)。在这些就诊中,39.7%(95%CI,37.1%-42.3%)接受 ED 级护理:24.5%(95%CI,21.7%-27.4%)最初被分诊为紧急或紧急,26.0%(95%CI,23.8%-28.3%)接受了 2 项或更多诊断性检查。这些拒绝诊断就诊与 87.9%(95%CI,87.3%-88.4%)的商业保险成年 ED 就诊(28304 例就诊中的 24882 例)(平均[SD]患者年龄为 38.5[14.1]岁;14362[57.9%]为女性,17483[68.7%]为白人)有相同的就诊症状。在这些拒绝症状就诊中,65.1%(95%CI,63.4%-66.9%)接受 ED 级护理:43.2%(95%CI,40.2%-46.4%)被分诊为紧急或紧急,51.9%(95%CI,40.0%-53.9%)接受了 2 项或更多诊断性检查,9.7%(95%CI,8.8%-10.6%)住院或转院。
从患者的角度来看,Anthem 的非紧急 ED 出院诊断与识别不必要的 ED 就诊无关。这项降低成本的政策可能会使许多合理寻求 ED 护理的患者面临承保拒绝的风险。