Department of Orthopedics, Clinical Sciences Lund, Lund University, Sweden.
BMC Musculoskelet Disord. 2009 Dec 8;10:154. doi: 10.1186/1471-2474-10-154.
The association between knee alignment and knee pain in knee osteoarthritis (OA) is unclear. High tibial osteotomy, a treatment option in knee OA, alters load from the affected to the unaffected compartment of the knee by correcting malalignment. This surgical procedure thus offers the possibility to study the cross-sectional and longitudinal association of alignment to pain. The aims were to study 1) the preoperative association of knee alignment to preoperative knee pain and 2) the association of change in knee alignment with surgery to change in knee pain over time in patients operated on for knee OA by high tibial osteotomy.
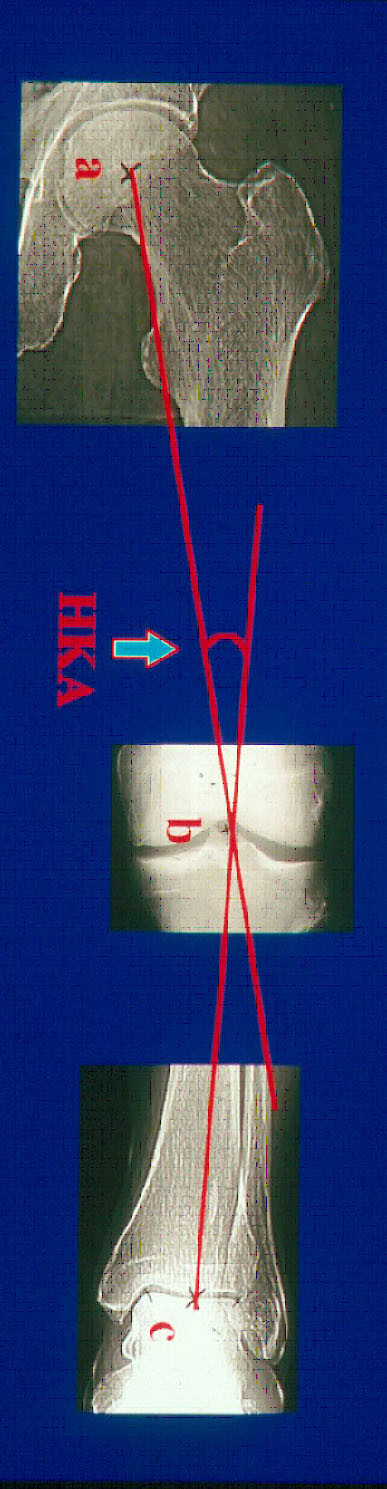
182 patients (68% men) mean age 53 years (34 - 69) with varus alignment having tibial osteotomy by the hemicallotasis technique for medial knee OA were consecutively included. Knee alignment was assessed by the Hip-Knee-Ankle (HKA) angle from radiographs including the hip and ankle joints. Knee pain was measured by the subscale pain (0 - 100, worst to best scale) of the Knee injury and Osteoarthritis Outcome Score (KOOS) preoperatively and at one year follow-up. To estimate the association between knee alignment and knee pain multivariate regression analyses were used.
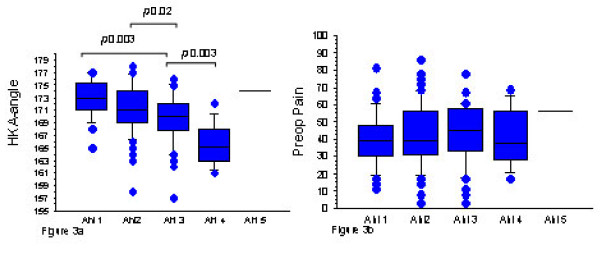
Mean preoperative varus alignment was 170 degrees (153 - 178) and mean preoperative KOOS pain was 42 points (3 - 86). There was no association between preoperative varus alignment and preoperative KOOS pain, crude analysis 0.02 points (95% CI -0.6 - 0.7) change in pain with every degree of HKA angle, adjusted analysis 0.3 points (95% CI -1.3 - 0.6).The mean postoperative knee alignment was 184 degrees (171 - 185). The mean change in knee alignment was 13 degrees (0 - 30). The mean change in KOOS pain was 32 (-16 - 83). There was neither any association between change in knee alignment and change in KOOS pain over time, crude analysis 0.3 point (95% CI -0.6 - 1.2), adjusted analysis 0.4 points (95% CI 0.6 - 1.4).
We found no association between knee alignment and knee pain in patients with knee OA indicating that alignment and pain are separate entities, and that the degree of preoperative malalignment is not a predictor of knee pain after high tibial osteotomy.
膝关节对线与膝骨关节炎(OA)患者膝关节疼痛之间的关系尚不清楚。胫骨高位截骨术是一种治疗膝 OA 的方法,通过纠正对线不良,将负荷从患病部位转移到未患病部位。因此,这种手术为研究对线与疼痛的横断面和纵向关联提供了可能性。目的是研究 1)术前膝关节对线与术前膝关节疼痛的关系,2)胫骨高位截骨术改变膝关节对线与随时间推移膝关节疼痛变化的关系。
连续纳入 182 例(68%为男性)平均年龄 53 岁(34-69)的内翻畸形患者,采用半骺离断技术行胫骨高位截骨术治疗内侧膝 OA。膝关节对线通过包括髋关节和踝关节的 X 线片的 Hip-Knee-Ankle(HKA)角评估。膝关节疼痛采用膝关节损伤和骨关节炎结果评分(KOOS)的子量表疼痛(0-100,最差到最好量表)测量,术前和 1 年随访时测量。为了评估膝关节对线与膝关节疼痛之间的关系,采用多元回归分析。
术前平均内翻畸形为 170 度(153-178),术前 KOOS 疼痛平均为 42 分(3-86)。术前内翻对线与术前 KOOS 疼痛之间无相关性,粗略分析为 0.02 点(95%CI-0.6-0.7),HKA 角度每度变化 0.3 点(95%CI-1.3-0.6)。术后平均膝关节对线为 184 度(171-185)。膝关节对线平均变化 13 度(0-30)。KOOS 疼痛平均变化 32 分(-16-83)。随时间推移,膝关节对线变化与 KOOS 疼痛变化之间也无相关性,粗略分析为 0.3 点(95%CI-0.6-1.2),调整分析为 0.4 点(95%CI 0.6-1.4)。
我们发现膝 OA 患者膝关节对线与膝关节疼痛之间无相关性,这表明对线和疼痛是两个独立的实体,术前对线不良的程度不是胫骨高位截骨术后膝关节疼痛的预测因素。