Department of Laboratory Medicine & Pathobiology, University of Toronto, 81A Resources Road, Rm 243, Toronto ON M9P 3T1, ON, Canada.
Malar J. 2009 Dec 9;8:284. doi: 10.1186/1475-2875-8-284.
Accurate laboratory diagnosis of malaria species in returning travelers is paramount in the treatment of this potentially fatal infectious disease.
A total of 466 blood specimens from returning travelers to Africa, Asia, and South/Central America with suspected malaria infection were collected between 2007 and 2009 at the reference public health laboratory. These specimens were assessed by reference microscopy, multipex real-time quantitative polymerase chain reaction (QPCR), and two rapid diagnostic immuno-chromatographic tests (ICT) in a blinded manner. Key clinical laboratory parameters such as limit of detection (LOD) analysis on clinical specimens by parasite stage, inter-reader variability of ICTs, staffing implications, quality assurance and cost analysis were evaluated.
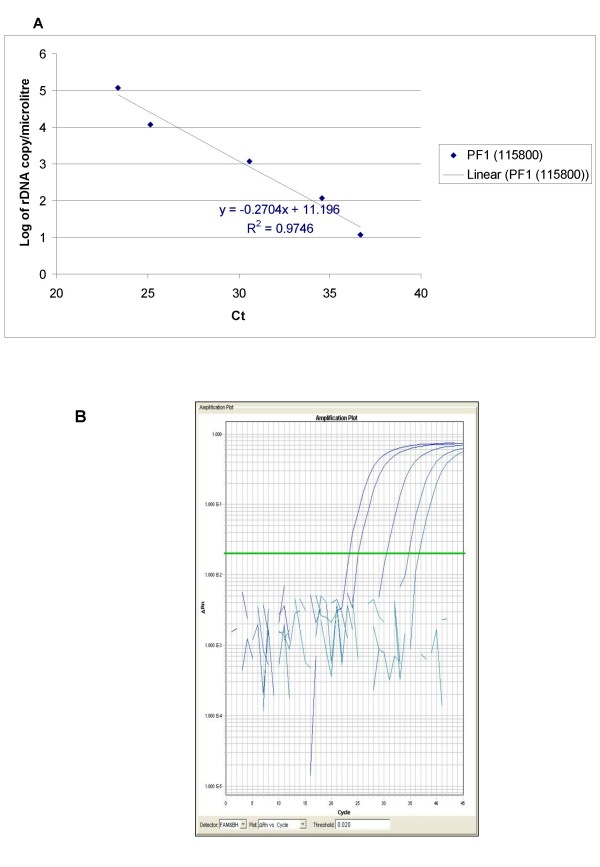
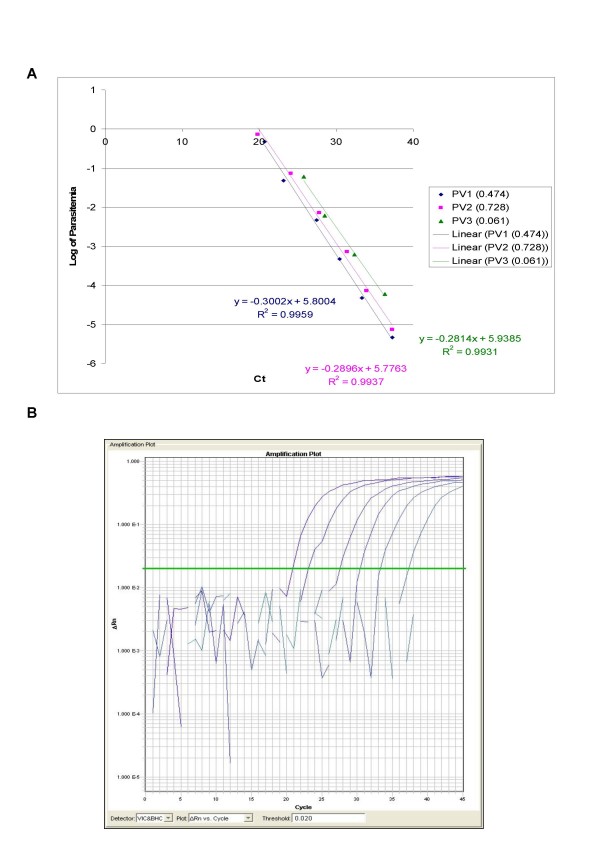
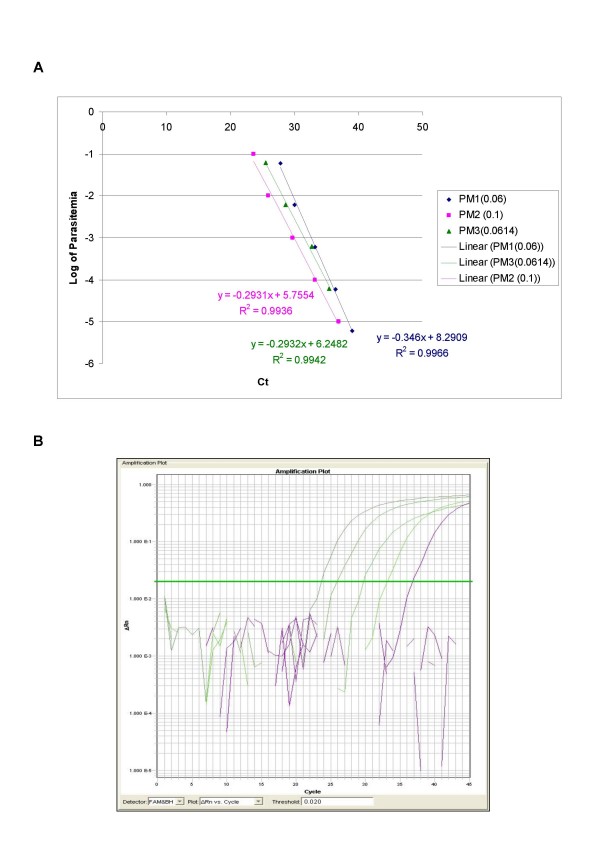
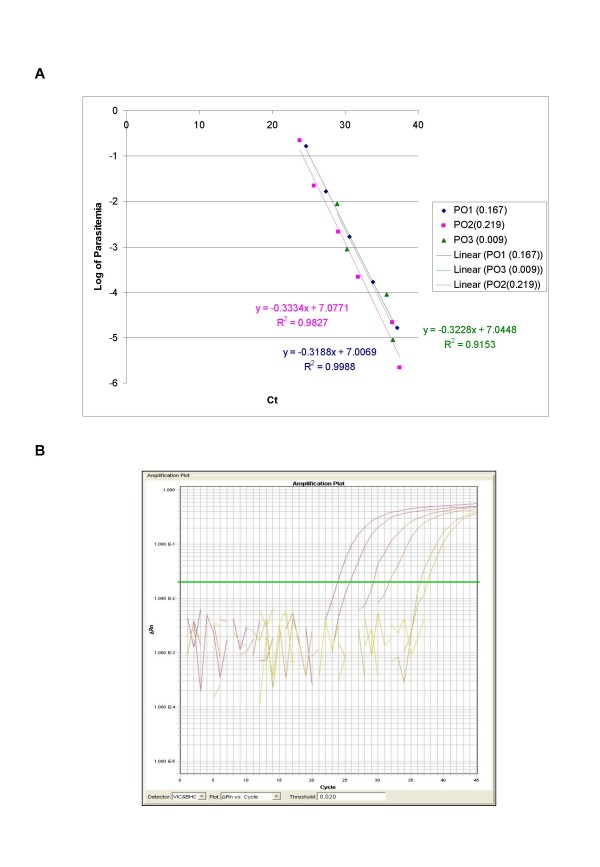
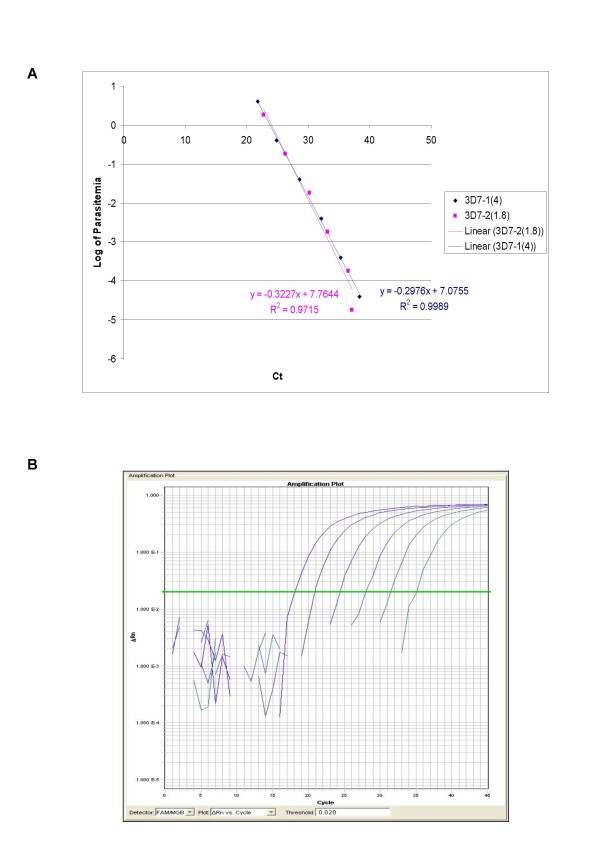
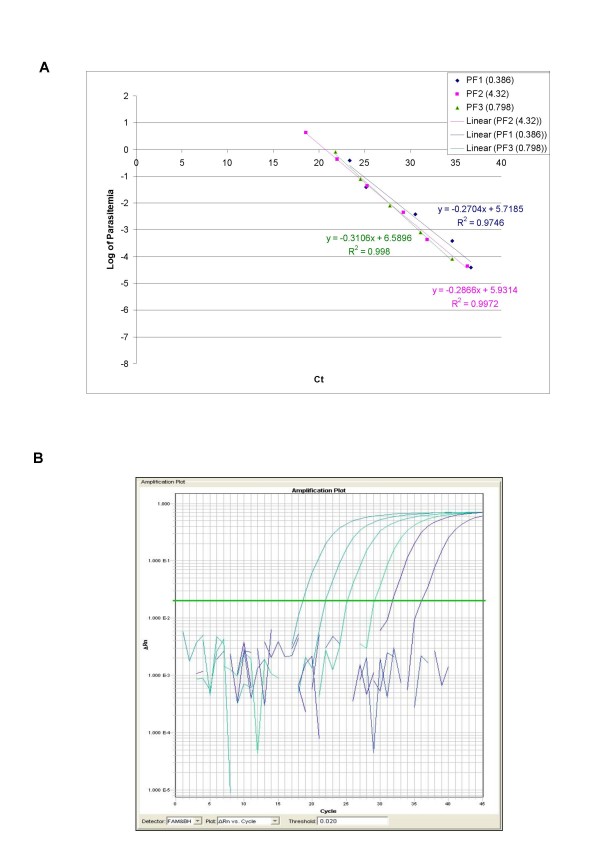
QPCR is the most analytically sensitive method (sensitivity 99.41%), followed by CARESTART (sensitivity 88.24%), and BINAXNOW (sensitivity 86.47%) for the diagnosis of malaria in returning travelers when compared to reference microscopy. However, microscopy was unable to specifically identify Plasmodia spp. in 18 out of 170 positive samples by QPCR. Moreover, the 17 samples that were negative by microscopy and positive by QPCR were also positive by ICTs. Quality assurance was achieved for QPCR by exchanging a blinded proficiency panel with another reference laboratory. The Kappa value of inter-reader variability among three readers for BINAXNOW and CARESTART was calculated to be 0.872 and 0.898 respectively. Serial dilution studies demonstrated that the QPCR cycle threshold correlates linearly with parasitemia (R(2) = 0.9746) in a clinically relevant dynamic range and retains a LOD of 11 rDNA copies/microl for P. falciparum, which was several log lower than reference microscopy and ICTs. LOD for QPCR is affected not only by parasitemia but the parasite stage distribution of each clinical specimen. QPCR was approximately 6-fold more costly than reference microscopy.
These data suggest that multiplex QPCR although more costly confers a significant diagnostic advantage in terms of LOD compared to reference microscopy and ICTs for all four species. Quality assurance of QPCR is essential to the maintenance of proficiency in the clinical laboratory. ICTs showed good concordance between readers however lacked sensitivity for non-falciparum species due to antigenic differences and low parasitemia.
Multiplex QPCR but not ICTs is an essential adjunct to microscopy in the reference laboratory detection of malaria species specifically due to the superior LOD. ICTs are better suited to the non-reference laboratory where lower specimen volumes challenge microscopy proficiency in the non-endemic setting.
在治疗这种潜在致命的传染病时,准确地对返回家园的旅行者中的疟疾病原种类进行实验室诊断至关重要。
2007 年至 2009 年间,在参考公共卫生实验室共采集了 466 份来自非洲、亚洲和南美/中美地区的疑似疟疾感染的返回家园旅行者的血液样本。这些标本通过参考显微镜检查、多重实时定量聚合酶链反应(QPCR)和两种快速诊断免疫层析检测(ICT)进行盲法评估。评估了关键的临床实验室参数,例如寄生虫阶段的临床标本检测限(LOD)分析、ICT 之间的读者间变异性、人员配备影响、质量保证和成本分析。
与参考显微镜相比,QPCR 是最具分析敏感性的方法(灵敏度 99.41%),其次是 CARESTART(灵敏度 88.24%)和 BINAXNOW(灵敏度 86.47%),用于诊断返回家园的旅行者中的疟疾。然而,显微镜无法在 170 个由 QPCR 检测为阳性的样本中特异性识别疟原虫属。此外,17 个由显微镜检测为阴性但由 QPCR 检测为阳性的样本也由 ICT 检测为阳性。通过与另一个参考实验室交换盲法能力验证小组,实现了 QPCR 的质量保证。三位读者对 BINAXNOW 和 CARESTART 的读者间变异性的 Kappa 值分别计算为 0.872 和 0.898。系列稀释研究表明,QPCR 的循环阈值与寄生虫血症呈线性相关(R²=0.9746),在临床相关的动态范围内,保留了对 11 个 rDNA 拷贝/微升的 P. falciparum 的检测限,这比参考显微镜和 ICT 低几个对数级。QPCR 的检测限不仅受寄生虫血症影响,还受每个临床标本中寄生虫阶段分布的影响。QPCR 的成本大约比参考显微镜高 6 倍。
这些数据表明,尽管多重 QPCR 成本更高,但与参考显微镜和 ICT 相比,在 LOD 方面具有显著的诊断优势,可用于检测所有四种疟原虫。QPCR 的质量保证对于维持临床实验室的能力至关重要。ICT 之间的读者之间具有良好的一致性,但是由于抗原差异和低寄生虫血症,对非恶性疟原虫物种缺乏敏感性。
多重 QPCR 而不是 ICT 是参考实验室检测疟原虫种类的显微镜的重要补充,这主要是因为其具有优越的 LOD。ICT 更适合非参考实验室,在非流行地区,较低的标本量会挑战显微镜的能力。