University of Birmingham, Edgbaston, UK.
Crit Care. 2009;13 Suppl 2(Suppl 2):S1. doi: 10.1186/cc7868.
This report describes the case mix and outcomes of patients with oesophageal cancer admitted to adult critical care units following elective oesophageal surgery in England, Wales and Northern Ireland.
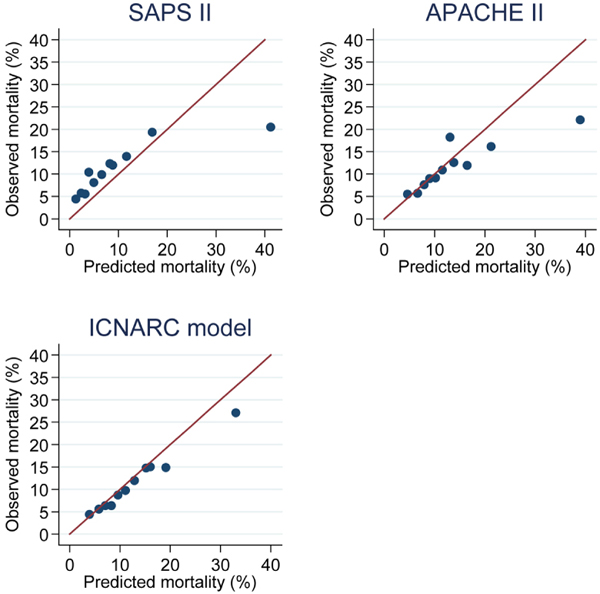
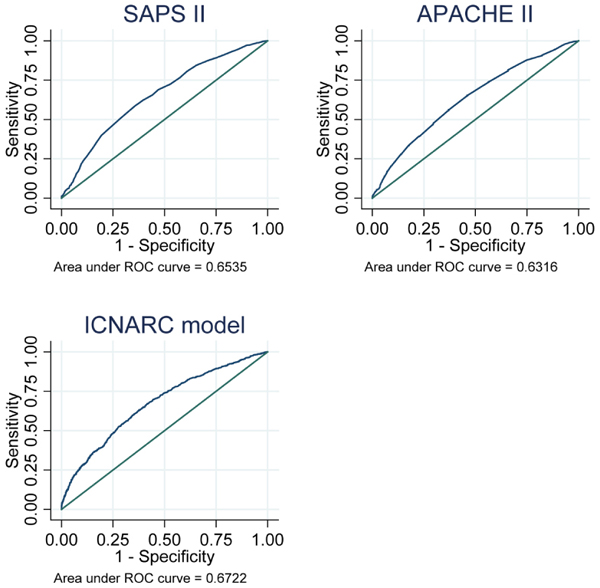
Admissions to critical care following elective oesophageal surgery for malignancy were identified using data from the Intensive Care National Audit and Research Centre (ICNARC) Case Mix Programme Database. Information on admissions between December 1995 and September 2007 were extracted and the association between in-hospital mortality and patient characteristics on admission to critical care was assessed using multiple logistic regression analysis. The performance of three prognostic models (Simplified Acute Physiology Score (SAPS) II, Acute Physiology and Chronic Health Evaluation (APACHE) II and the ICNARC physiology score) was also evaluated.
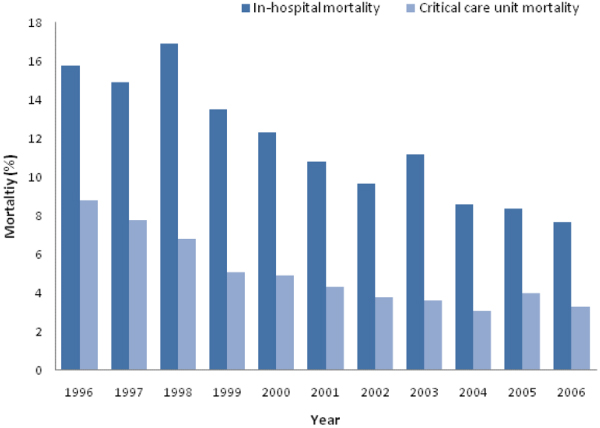
Between 1995 and 2007, there were 7227 admissions to 181 critical care units following oesophageal surgery for malignancy. Overall mortality in critical care was 4.4% and in-hospital mortality was 11%, although both declined steadily over time. Eight hundred and seventy-three (12.2%) patients were readmitted to critical care, most commonly for respiratory complications (49%) and surgical complications (25%). Readmitted patients had a critical care unit mortality of 24.7% and in-hospital mortality of 33.9%. Overall in-hospital mortality was associated with patient age, and various physiological measurements on admission to critical care (partial pressure of arterial oxygen (PaO2):fraction of inspired oxygen (FiO2) ratio, lowest arterial pH, mechanical ventilation, serum albumin, urea and creatinine). The three prognostic models evaluated performed poorly in measures of discrimination, calibration and goodness of fit.
Surgery for oesophageal malignancy continues to be associated with significant morbidity and mortality. Age and organ dysfunction in the early postoperative period are associated with an increased risk of death. Postoperative serum albumin is confirmed as an additional prognostic factor. More work is required to determine how this knowledge may improve clinical management.
本报告描述了英格兰、威尔士和北爱尔兰接受择期食管手术的成年重症监护病房(CCU)中接受治疗的食管癌患者的病例组合和结局。
使用重症监护国家审计和研究中心(ICNARC)病例组合计划数据库中的数据,确定择期食管恶性肿瘤手术后入住 CCU 的患者。提取 1995 年 12 月至 2007 年 9 月之间的入院信息,并使用多变量逻辑回归分析评估 CCU 入院时患者特征与院内死亡率之间的关系。还评估了三个预后模型(简化急性生理学评分(SAPS)II、急性生理学和慢性健康评估(APACHE)II 和 ICNARC 生理学评分)的性能。
1995 年至 2007 年间,有 7227 名接受恶性食管手术后的患者被转入 181 个 CCU。CCU 内的总死亡率为 4.4%,院内死亡率为 11%,尽管这两个数字都在稳步下降。873 名(12.2%)患者再次入住 CCU,最常见的原因是呼吸并发症(49%)和手术并发症(25%)。再次入住 CCU 的患者 CCU 死亡率为 24.7%,院内死亡率为 33.9%。总的院内死亡率与患者年龄以及 CCU 入院时的各种生理指标(动脉血氧分压(PaO2)与吸入氧分数(FiO2)比值、最低动脉 pH 值、机械通气、血清白蛋白、尿素和肌酐)有关。评估的三个预后模型在区分度、校准度和拟合优度方面表现不佳。
食管恶性肿瘤手术仍然与显著的发病率和死亡率相关。术后早期的年龄和器官功能障碍与死亡风险增加相关。术后血清白蛋白被确认为另一个预后因素。需要进一步研究以确定如何利用这些知识来改善临床管理。