Department of Obstetrics and Gynaecology, Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands.
BMC Womens Health. 2009 Dec 18;9:35. doi: 10.1186/1472-6874-9-35.
Multiple pregnancies are high risk pregnancies with higher chances of maternal and neonatal mortality and morbidity. In the past decades the number of multiple pregnancies has increased. This trend is partly due to the fact that women start family planning at an increased age, but also due to the increased use of ART.Couples with unexplained or mild male subfertility generally receive intrauterine insemination IUI with controlled hormonal stimulation (IUI COH). The cumulative pregnancy rate is 40%, with a 10% multiple pregnancy rate.This study aims to reveal whether alternative treatments such as IVF elective Single Embryo Transfer (IVF e SET) or Modified Natural Cycle IVF (MNC IVF) can reduce the number of multiple pregnancy rates, but uphold similar pregnancy rates as IUI COH in couples with mild male or unexplained subfertility. Secondly, the aim is to perform a cost effective analyses and assess treatment preference of these couples.
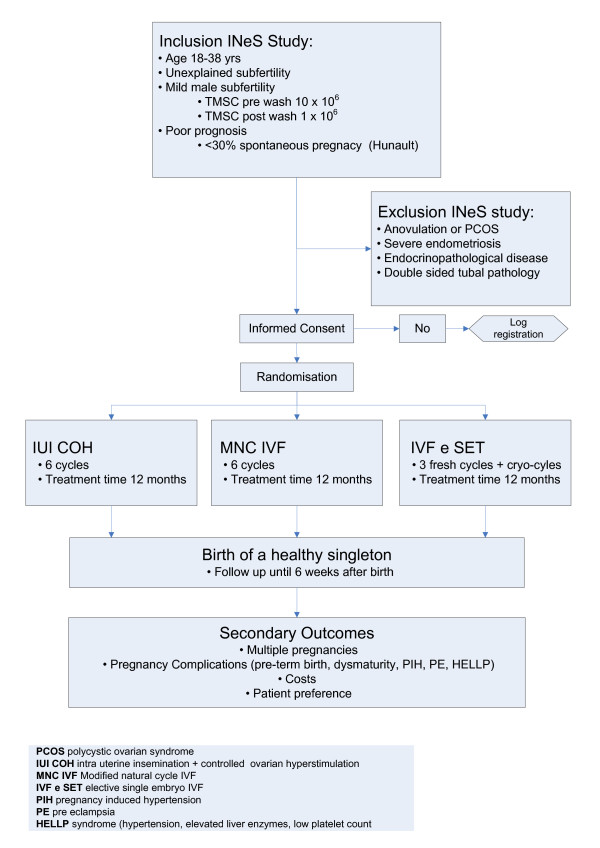
METHODS/DESIGN: We plan a multicentre randomised controlled clinical trial in the Netherlands comparing six cycles of intra-uterine insemination with controlled ovarian hyperstimulation or six cycles of Modified Natural Cycle (MNC) IVF or three cycles with IVF-elective Single Embryo Transfer (eSET) plus cryo-cycles within a time frame of 12 months.Couples with unexplained subfertility or mild male subfertility and a poor prognosis for treatment independent pregnancy will be included. Women with anovulatory cycles, severe endometriosis, double sided tubal pathology or serious endocrine illness will be excluded.Our primary outcome is the birth of a healthy singleton. Secondary outcomes are multiple pregnancy, treatment costs, and patient experiences in each treatment arm. The analysis will be performed according tot the intention to treat principle. We will test for non-inferiority of the three arms with respect to live birth. As we accept a 12.5% loss in pregnancy rate in one of the two IVF arms to prevent multiple pregnancies, we need 200 couples per arm (600 couples in total).
Determining the safest and most cost-effective treatment will ensure optimal chances of pregnancy for subfertile couples with substantially diminished perinatal and maternal complications. Should patients find the most cost-effective treatment acceptable or even preferable, this could imply the need for a world wide shift in the primary treatment.
Current Controlled Trials ISRCTN 52843371.
多胎妊娠是高危妊娠,母婴死亡率和发病率较高。在过去几十年中,多胎妊娠的数量有所增加。这种趋势部分归因于女性开始计划生育的年龄增加,但也归因于辅助生殖技术(ART)的使用增加。不明原因或轻度男性不育的夫妇通常接受宫腔内人工授精(IUI)联合控制性激素刺激(IUI COH)。累积妊娠率为 40%,多胎妊娠率为 10%。本研究旨在探讨替代治疗方法,如体外受精选择性单胚胎移植(IVF eSET)或改良自然周期 IVF(MNC IVF),是否可以降低多胎妊娠率,同时保持不明原因或轻度男性不育夫妇的 IUI COH 相似的妊娠率。其次,目的是进行成本效益分析,并评估这些夫妇的治疗偏好。
方法/设计:我们计划在荷兰进行一项多中心随机对照临床试验,比较 6 个周期的宫腔内人工授精联合控制性卵巢过度刺激或 6 个周期的改良自然周期(MNC)IVF 或 3 个周期的 IVF 选择性单胚胎移植(eSET)联合冷冻周期,时间框架为 12 个月。纳入不明原因不孕或轻度男性不育且独立妊娠预后不佳的夫妇。排除无排卵周期、严重子宫内膜异位症、双侧输卵管病变或严重内分泌疾病的妇女。我们的主要结局是健康单胎的分娩。次要结局是多胎妊娠、治疗成本以及每个治疗组的患者体验。分析将根据意向治疗原则进行。我们将根据活产率对三个手臂进行非劣效性检验。由于我们接受两个 IVF 手臂中的一个妊娠率降低 12.5%以防止多胎妊娠,因此每个手臂需要 200 对夫妇(总共 600 对夫妇)。
确定最安全和最具成本效益的治疗方法将确保有生育问题的夫妇有最佳的妊娠机会,同时大大降低围产期和母婴并发症的风险。如果患者认为最具成本效益的治疗方法可以接受甚至更可取,这可能意味着需要在全球范围内改变主要治疗方法。
当前对照试验 ISRCTN52843371。