Centre for Reproductive Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam 1105 AZ, the Netherlands.
Centre for Reproductive Medicine, University Medical Centre Utrecht, Utrecht 3508 GA, the Netherlands.
Hum Reprod. 2021 Feb 18;36(3):817-825. doi: 10.1093/humrep/deaa298.
Does assisted reproduction, such as ovarian stimulation and/or laboratory procedures, have impact on perinatal outcomes of singleton live births compared to natural conception in couples with unexplained subfertility?
Compared to natural conception, singletons born after intrauterine insemination with ovarian stimulation (IUI-OS) had a lower birthweight, while singletons born after IVF had comparable birthweights, in couples with unexplained subfertility.
Singletons conceived by assisted reproduction have different perinatal outcomes such as low birthweight and a higher risk of premature birth than naturally conceived singletons. This might be due to the assisted reproduction, such as laboratory procedures or the ovarian stimulation, or to an intrinsic factor in couples with subfertility.
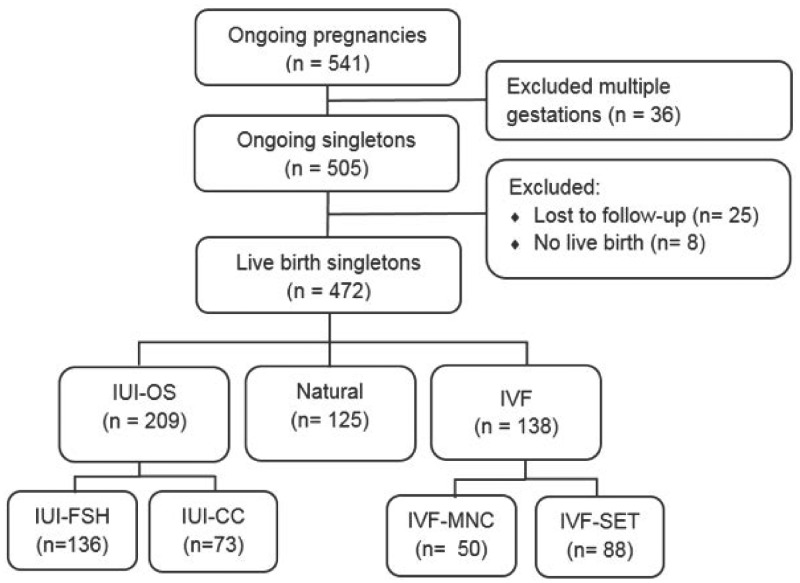
STUDY DESIGN, SIZE, DURATION: We performed a prospective cohort study using the follow-up data of two randomized clinical trials performed in couples with unexplained subfertility. We evaluated perinatal outcomes of 472 live birth singletons conceived after assisted reproduction or after natural conception within the time horizon of the studies.
PARTICIPANTS/MATERIALS, SETTING, METHODS: To assess the possible impact of ovarian stimulation we compared the singletons conceived after IUI with FSH or clomiphene citrate (CC) and IVF in a modified natural cycle (IVF-MNC) or standard IVF with single embryo transfer (IVF-SET) to naturally conceived singletons in the same cohorts. To further look into the possible effect of the laboratory procedures, we put both IUI and IVF groups together into IUI-OS and IVF and compared both to singletons born after natural conception. We only included singletons conceived after fresh embryo transfers. The main outcome was birthweight presented as absolute weight in grams and gestational age- and gender-adjusted percentiles. We calculated differences in birthweight using regression analyses adjusted for maternal age, BMI, smoking, parity, duration of subfertility and child gender.
In total, there were 472 live birth singletons. Of the 472 singleton pregnancies, 209 were conceived after IUI-OS (136 with FSH and 73 with CC as ovarian stimulation), 138 after IVF (50 after IVF-MNC and 88 after IVF-SET) and 125 were conceived naturally.Singletons conceived following IUI-FSH and IUI-CC both had lower birthweights compared to naturally conceived singletons (adjusted difference IUI-FSH -156.3 g, 95% CI -287.9 to -24.7; IUI-CC -160.3 g, 95% CI -316.7 to -3.8). When we compared IVF-MNC and IVF-SET to naturally conceived singletons, no significant difference was found (adjusted difference IVF-MNC 75.8 g, 95% CI -102.0 to 253.7; IVF-SET -10.6 g, 95% CI -159.2 to 138.1). The mean birthweight percentile was only significantly lower in the IUI-FSH group (-7.0 percentile, 95% CI -13.9 to -0.2). The IUI-CC and IVF-SET group had a lower mean percentile and the IVF-MNC group a higher mean percentile, but these groups were not significant different compared to the naturally conceived group (IUI-CC -5.1 percentile, 95% CI -13.3 to 3.0; IVF-MNC 4.4 percentile, 95% CI -4.9 to 13.6; IVF-SET -1.3 percentile, 95% CI -9.1 to 6.4).Looking at the laboratory process that took place, singletons conceived following IUI-OS had lower birthweights than naturally conceived singletons (adjusted difference -157.7 g, 95% CI -277.4 to -38.0). The IVF group had comparable birthweights with the naturally conceived group (adjusted difference 20.9 g, 95% CI -110.8 to 152.6). The mean birthweight percentile was significantly lower in the IUI-OS group compared to the natural group (-6.4 percentile, 95% CI -12.6 to -0.1). The IVF group was comparable (0.7 percentile, 95% CI -6.1 to 7.6).
LIMITATIONS, REASONS FOR CAUTION: The results are limited by the number of cases. The data were collected prospectively alongside the randomized controlled trials, but analyzed as treated.
Our data suggest IUI in a stimulated cycle may have a negative impact on the birthweight of the child and possibly on pre-eclampsia. Further research should look into the effect of different methods of ovarian stimulation on placenta pathology and pre-eclampsia in couples with unexplained subfertility using naturally conceived singletons in the unexplained population as a reference.
STUDY FUNDING/COMPETING INTEREST(S): Both initial trials were supported by a grant from ZonMW, the Dutch Organization for Health Research and Development (INeS 120620027, SUPER 80-83600-98-10192). The INeS study also had a grant from Zorgverzekeraars Nederland, the Dutch association of healthcare insurers (09-003). B.W.J.M. is supported by an NHMRC investigator Grant (GNT1176437) and reports consultancy for ObsEva, Merck Merck KGaA, Guerbet and iGenomix, outside the submitted work. A.H. reports grants from Ferring Pharmaceutical company (the Netherlands), outside the submitted work. F.J.M.B. receives monetary compensation as a member of the external advisory board for Merck Serono (the Netherlands), Ferring Pharmaceutics BV (the Netherlands) and Gedeon Richter (Belgium), he receives personal fees from educational activities for Ferring BV (the Netherlands) and for advisory and consultancy work for Roche and he receives research support grants from Merck Serono and Ferring Pharmaceutics BV, outside the submitted work. The remaining authors have nothing to disclose.
INeS study Trial NL915 (NTR939); SUPER Trial NL3895 (NTR4057).
与不明原因不孕的夫妇自然受孕相比,卵巢刺激和/或实验室程序等辅助生殖是否会影响单胎活产儿的围产期结局?
与自然受孕相比,接受宫腔内人工授精加卵巢刺激(IUI-OS)的单胎婴儿出生体重较低,而接受体外受精(IVF)的单胎婴儿出生体重相当,在不明原因不孕的夫妇中。
通过辅助生殖技术受孕的单胎婴儿与自然受孕的单胎婴儿相比,具有不同的围产期结局,如低出生体重和早产风险增加。这可能是由于辅助生殖技术,如实验室程序或卵巢刺激,或由于不孕夫妇的内在因素。
研究设计、大小、持续时间:我们使用两项不明原因不孕夫妇进行的随机临床试验的随访数据进行了前瞻性队列研究。我们评估了研究时间范围内辅助生殖或自然受孕后 472 例活产单胎的围产期结局。
参与者/材料、设置、方法:为了评估卵巢刺激的可能影响,我们将接受 FSH 或克罗米酚(CC)刺激的 IUI 与改良自然周期(IVF-MNC)或标准 IVF 与单胚胎转移(IVF-SET)的 IVF 与同一队列中的自然受孕的单胎进行了比较。为了进一步研究实验室程序的可能影响,我们将 IUI 和 IVF 两组都归入 IUI-OS 和 IVF 组,并将其与自然受孕的单胎进行了比较。我们仅纳入了新鲜胚胎移植后受孕的单胎。主要结局是出生体重,以克为单位绝对体重和胎龄及性别调整的百分位数表示。我们使用回归分析计算出生体重差异,调整了母亲年龄、BMI、吸烟、产次、不孕持续时间和儿童性别。
共有 472 例活产单胎。在 472 例单胎妊娠中,209 例经 IUI-OS 受孕(136 例用 FSH,73 例用 CC 作为卵巢刺激),138 例经 IVF 受孕(50 例经 IVF-MNC,88 例经 IVF-SET),125 例自然受孕。接受 IUI-FSH 和 IUI-CC 的单胎婴儿的出生体重均低于自然受孕的单胎婴儿(调整差异 IUI-FSH-156.3g,95%CI-287.9 至-24.7;IUI-CC-160.3g,95%CI-316.7 至-3.8)。当我们将 IVF-MNC 和 IVF-SET 与自然受孕的单胎进行比较时,没有发现显著差异(调整差异 IVF-MNC75.8g,95%CI-102.0 至 253.7;IVF-SET-10.6g,95%CI-159.2 至 138.1)。只有 IUI-FSH 组的平均出生体重百分位数显著降低(-7.0 个百分点,95%CI-13.9 至-0.2)。IUI-CC 和 IVF-SET 组的平均百分位数较低,而 IVF-MNC 组的平均百分位数较高,但与自然受孕组相比,这些组均无显著差异(IUI-CC-5.1 个百分点,95%CI-13.3 至 3.0;IVF-MNC4.4 个百分点,95%CI-4.9 至 13.6;IVF-SET-1.3 个百分点,95%CI-9.1 至 6.4)。
观察实验室过程,IUI-OS 受孕的单胎婴儿的出生体重低于自然受孕的单胎婴儿(调整差异-157.7g,95%CI-277.4 至-38.0)。IVF 组与自然受孕组的出生体重相当(调整差异 20.9g,95%CI-110.8 至 152.6)。IUI-OS 组的平均出生体重百分位数明显低于自然组(-6.4 个百分点,95%CI-12.6 至-0.1)。IVF 组相当(0.7 个百分点,95%CI-6.1 至 7.6)。
局限性、谨慎的原因:结果受到病例数量的限制。这些数据是在与不明原因不孕的夫妇进行的两项随机对照试验的同时前瞻性收集的,但作为治疗进行了分析。
我们的数据表明,刺激周期中的 IUI 可能对儿童的出生体重产生负面影响,并可能对先兆子痫产生影响。进一步的研究应该使用不明原因不孕人群中的自然受孕单胎作为参考,研究不同的卵巢刺激方法对不明原因不孕夫妇胎盘病理学和先兆子痫的影响。
研究资金/利益冲突:两项初始试验均由 ZonMW(荷兰卫生研究与发展组织)资助(INeS120620027、SUPER80-83600-98-10192)。INeS 研究还得到了荷兰医疗保险公司(ZorgverzekeraarsNederland)的资助(09-003)。B.W.J.M. 得到了 NHMRC 研究员赠款(GNT1176437)的支持,并报告了对 ObsEva、Merck KGaA、Guerbet 和 iGenomix 的咨询工作,这些都与提交的工作无关。A.H. 报告从 FerringPharmaceutical 公司(荷兰)获得研究经费,从 Merck Serono(荷兰)、FerringPharmaceuticsBV(荷兰)和 Gedeon Richter(比利时)获得咨询费,从 Roche 获得教育活动的个人酬金,并从 Merck Serono 和 FerringPharmaceuticsBV 获得研究支持赠款,这些都与提交的工作无关。其余作者没有任何利益冲突。
INeS 研究 NL915(NTR939);SUPER 研究 NL3895(NTR4057)。