Department of Pharmacology and Experimental Neuroscience, University of Nebraska Medical Center, Omaha, NE 68198-5880, USA.
Neurobiol Dis. 2010 Mar;37(3):542-8. doi: 10.1016/j.nbd.2009.12.015. Epub 2010 Jan 4.
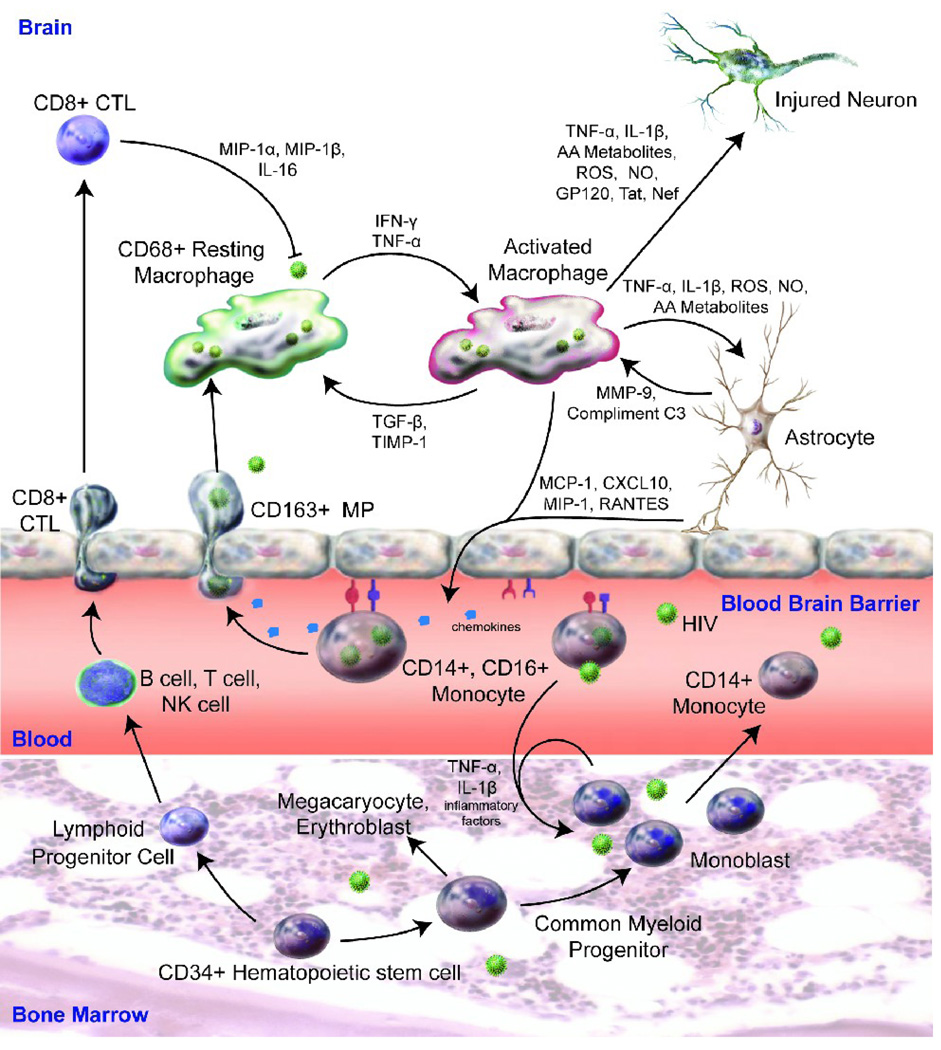
Human immunodeficiency virus type 1 (HIV-1)-associated neurocognitive disorders (HAND) can affect up to 50% of infected people during the disease course. While antiretroviral therapies have substantively increased the quality of life and reduced HIV-1-associated dementia, less severe minor cognitive and motor deficits continue. Trafficking of HIV-1 into the central nervous system (CNS), peripheral immune activation, dysregulated glial immunity, and diminished homeostatic responses are the disease-linked pathobiologic events. Monocyte-macrophage passage into the CNS remains an underlying force for disease severity. Monocyte phenotypes may change at an early stage of cell maturation and immune activation of hematopoietic stem cells. Activated monocytes are pulled into the brain in response to chemokines made as a result of glial inflammatory processes, which in turn, cause secondary functional deficits in neurons. Current therapeutic approaches are focused on adjunctive and brain-penetrating antiretroviral therapies. These may attenuate virus-associated neuroinflammatory activities thereby decreasing the severity and frequency of HAND.
人类免疫缺陷病毒 1 型(HIV-1)相关的神经认知障碍(HAND)可在疾病过程中影响多达 50%的感染者。虽然抗逆转录病毒疗法实质性地提高了生活质量并减少了与 HIV-1 相关的痴呆,但仍存在较轻的认知和运动功能减退。HIV-1 进入中枢神经系统(CNS)、外周免疫激活、神经胶质免疫失调以及稳态反应减弱是与疾病相关的病理生物学事件。HIV-1 从单核细胞-巨噬细胞向中枢神经系统的转移仍然是疾病严重程度的根本原因。单核细胞表型可能在细胞成熟和造血干细胞免疫激活的早期阶段发生变化。活化的单核细胞在趋化因子的作用下被拉进大脑,这些趋化因子是由神经胶质炎症过程产生的,反过来又导致神经元的继发性功能缺陷。目前的治疗方法侧重于辅助和穿透血脑屏障的抗逆转录病毒疗法。这些疗法可能减轻与病毒相关的神经炎症活动,从而降低 HAND 的严重程度和频率。