Department of Radiation Oncology, College for Public Health, Ohio State University, Columbus, OH 43210, USA.
Cancer. 2010 Feb 15;116(4):903-12. doi: 10.1002/cncr.24822.
The authors prospectively evaluated magnetic resonance imaging (MRI) parameters quantifying heterogeneous perfusion pattern and residual tumor volume early during treatment in cervical cancer, and compared their predictive power for primary tumor recurrence and cancer death with the standard clinical prognostic factors. A novel approach of augmenting the predictive power of clinical prognostic factors with MRI parameters was assessed.
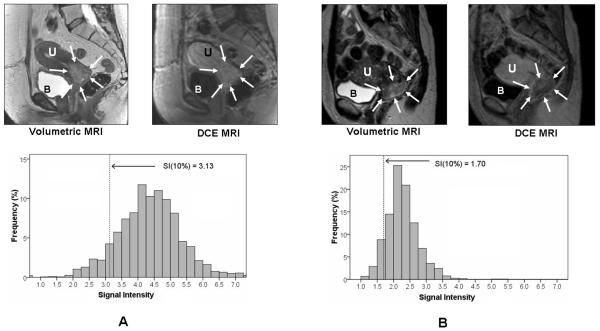
Sixty-two cervical cancer patients underwent dynamic contrast-enhanced (DCE) MRI before and during early radiation/chemotherapy (2-2.5 weeks into treatment). Heterogeneous tumor perfusion was analyzed by signal intensity (SI) of each tumor voxel. Poorly perfused tumor regions were quantified as lower 10th percentile of SI (SI[10%]). DCE-MRI and 3-dimensional (3D) tumor volumetry MRI parameters were assessed as predictors of recurrence and cancer death (median follow-up, 4.1 years). Their discriminating capacity was compared with clinical prognostic factors (stage, lymph node status, histology) using sensitivity/specificity and Cox regression analysis.
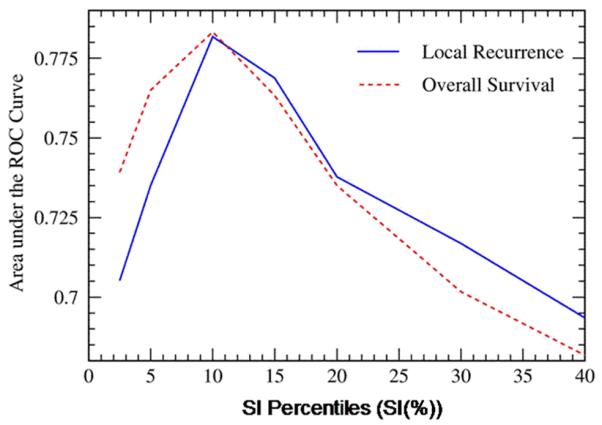
SI(10%) and 3D volume 2-2.5 weeks into therapy independently predicted disease recurrence (hazard ratio [HR], 2.6; 95% confidence interval [95% CI], 1.0-6.5 [P = .04] and HR, 1.9; 95% CI, 1.1-3.5 [P = .03], respectively) and death (HR, 1.9; 95% CI, 1.0-3.5 [P = .03] and HR, 1.9; 95% CI, 1.2-2.9 [P = .01], respectively), and were superior to clinical prognostic factors. The addition of MRI parameters to clinical prognostic factors increased sensitivity and specificity of clinical prognostic factors from 71% and 51%, respectively, to 100% and 71%, respectively, for predicting recurrence, and from 79% and 54%, respectively, to 93% and 60%, respectively, for predicting death.
MRI parameters reflecting heterogeneous tumor perfusion and subtle tumor volume change early during radiation/chemotherapy are independent and better predictors of tumor recurrence and death than clinical prognostic factors. The combination of clinical prognostic factors and MRI parameters further improves early prediction of treatment failure and may enable a window of opportunity to alter treatment strategy.
作者前瞻性评估了磁共振成像(MRI)参数,这些参数可量化宫颈癌治疗早期不均匀灌注模式和残留肿瘤体积,并将其预测原发性肿瘤复发和癌症死亡的能力与标准临床预后因素进行比较。评估了一种通过 MRI 参数增强临床预后因素预测能力的新方法。
62 例宫颈癌患者在放疗/化疗前(治疗开始后 2-2.5 周)和早期进行动态对比增强(DCE)MRI。通过每个肿瘤体素的信号强度(SI)分析不均匀肿瘤灌注。将灌注不良的肿瘤区域量化为 SI 的较低 10%(SI[10%])。DCE-MRI 和 3 维(3D)肿瘤体积 MRI 参数被评估为复发和癌症死亡的预测因子(中位随访时间为 4.1 年)。使用灵敏度/特异性和 Cox 回归分析将其区分能力与临床预后因素(分期、淋巴结状态、组织学)进行比较。
治疗 2-2.5 周时的 SI[10%]和 3D 体积独立预测疾病复发(危险比[HR],2.6;95%置信区间[95%CI],1.0-6.5[P=.04]和 HR,1.9;95%CI,1.1-3.5[P=.03])和死亡(HR,1.9;95%CI,1.0-3.5[P=.03]和 HR,1.9;95%CI,1.2-2.9[P=.01]),并且优于临床预后因素。将 MRI 参数添加到临床预后因素中,可将临床预后因素预测复发的灵敏度和特异性从 71%和 51%分别提高到 100%和 71%,预测死亡的灵敏度和特异性从 79%和 54%分别提高到 93%和 60%。
反映放疗/化疗早期不均匀肿瘤灌注和细微肿瘤体积变化的 MRI 参数是肿瘤复发和死亡的独立且更好的预测因素,优于临床预后因素。临床预后因素与 MRI 参数的结合可进一步提高治疗失败的早期预测能力,并可能为改变治疗策略提供机会窗口。