Roberts C S, Roberts W C
Surgery Branch, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, MD 20892.
Ann Surg. 1991 Apr;213(4):356-68. doi: 10.1097/00000658-199104000-00011.
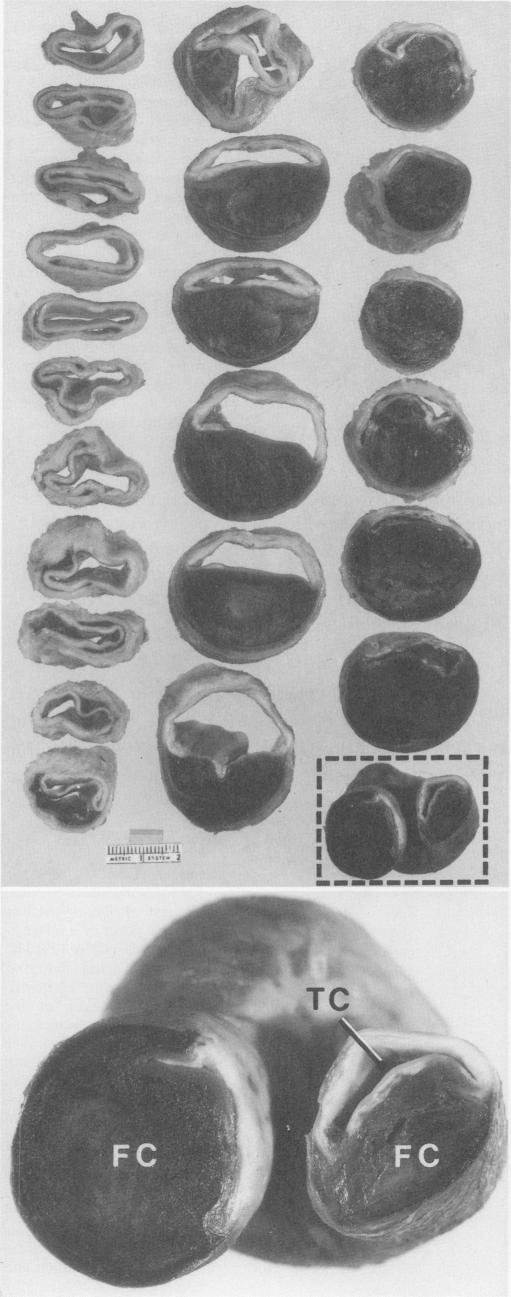
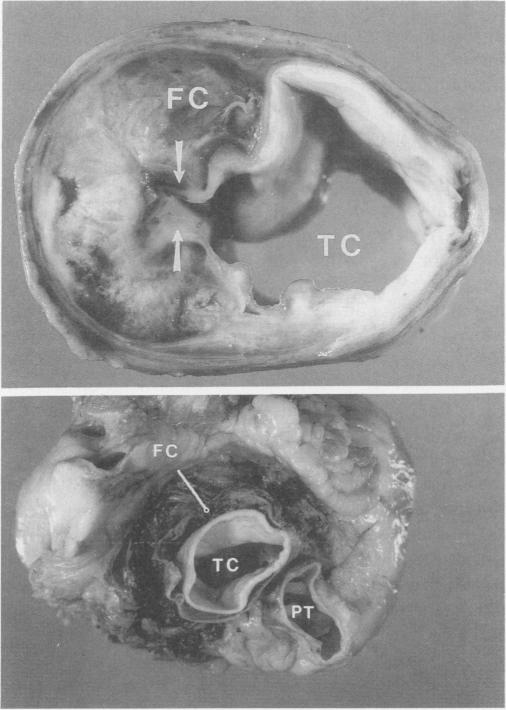
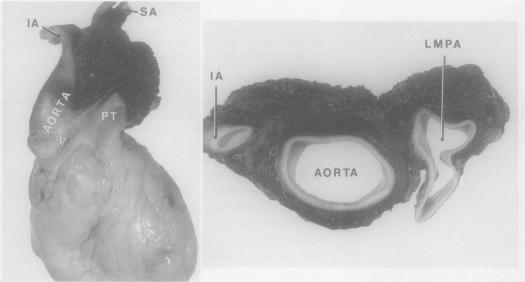
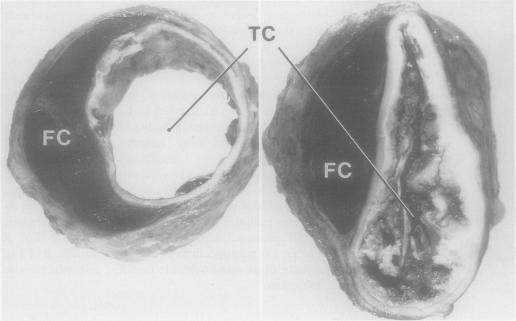
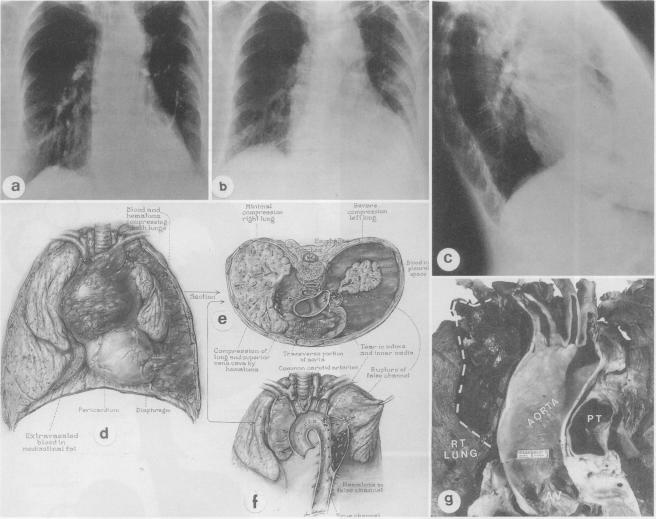
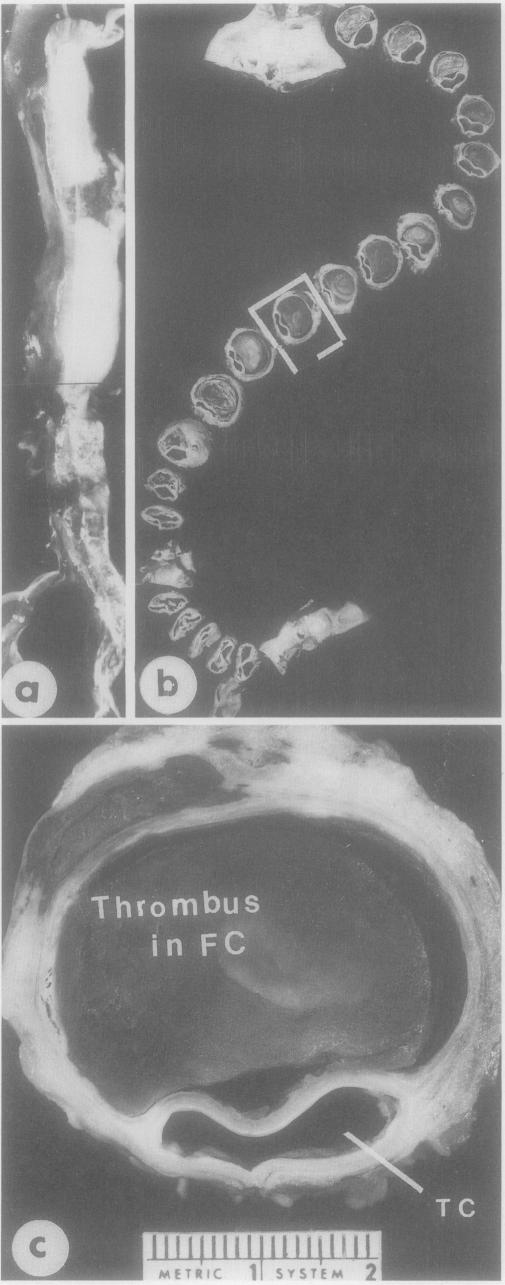
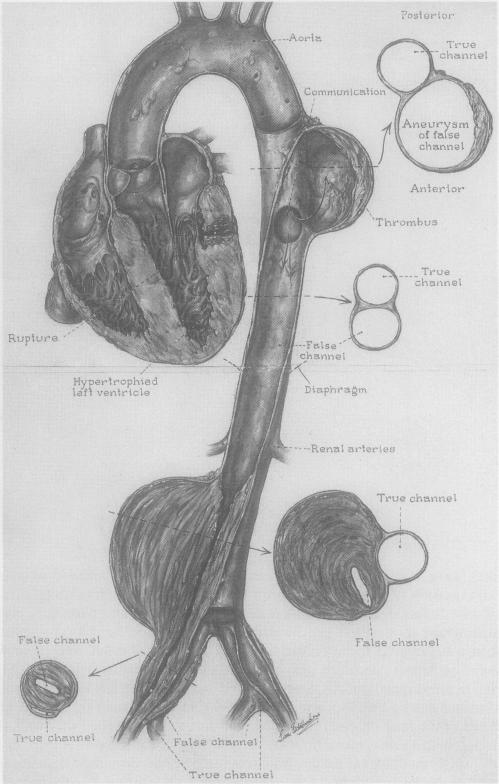
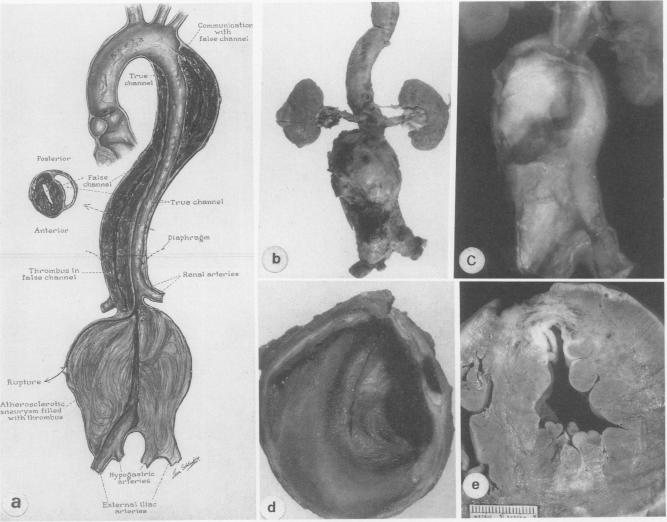
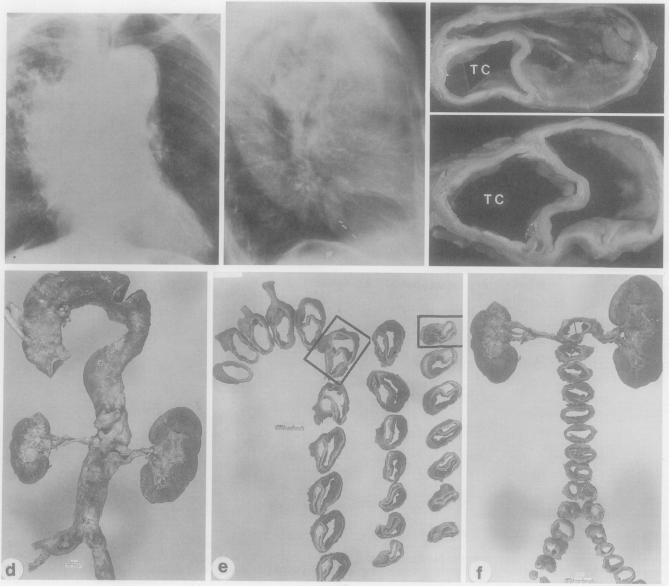
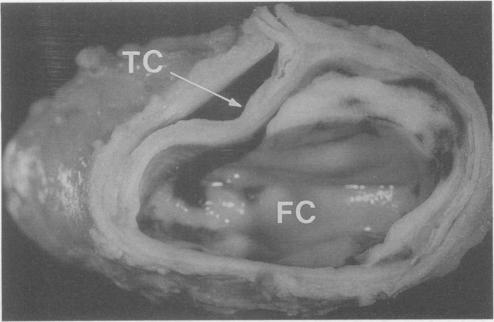
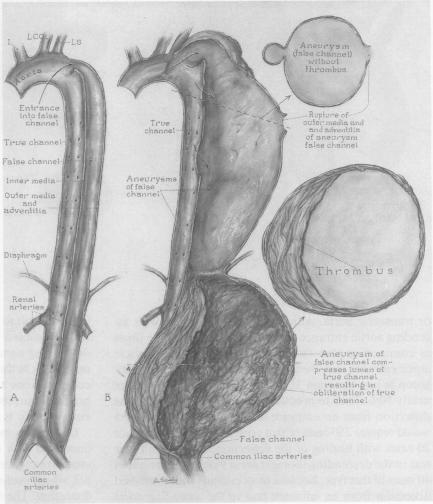
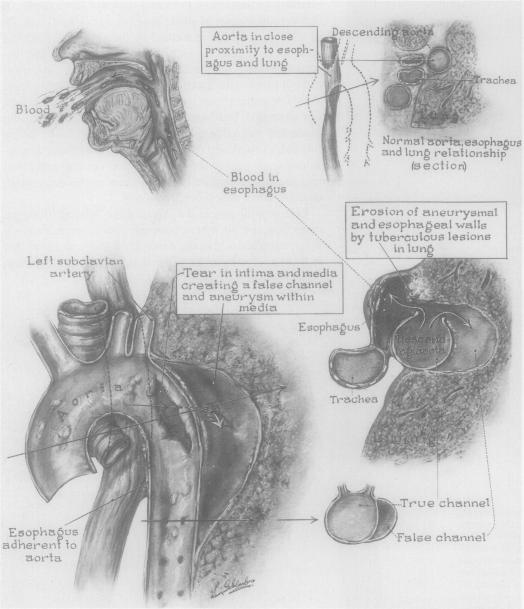
Clinical and necropsy findings are described in 40 patients who had aortic dissection with the entrance tear in the descending thoracic aorta. Their ages at death ranged from 39 to 91 years (mean, 66 years); 24 (60%) were men and 16 (40%) were women. Systemic hypertension was present by history in 33 patients (83%) and the hearts were of increased weight in 78%. Of the 40 patients, 31 (78%) had no operative intervention, while 9 (22%) underwent operation for aortic dissection. Of the 31 patients without operative therapy, the diagnosis of aortic dissection was established in life in 9 patients (29%) and at necropsy in 22 (71%). The interval from aortic dissection to death was 30 days or less in 13 patients (42%); rupture of the false channel was the cause of death in 9 patients (69%), renal failure in 2 (15%), and the cause was unclear in 2 (15%). The interval from aortic dissection to death was more than 30 days in 18 (58%) of the 31 patients without operative therapy. The cause of death in these 18 patients was related to the dissection in 11 (61%) (rupture of the false channel in 5; renal failure from dissection in 3, and rupture of the false channel of a second acute dissection in 3), but in the other 7 patients (39%) death was unrelated to the dissection but a nonfatal complication, specifically stenosis of the true channel from compression by a thrombus-filled false channel, occurred in 4 of these 7 patients. Thus only 3 (10%) of the 31 patients without operative therapy had no complications of aortic dissection. All nine patients who underwent operation had had an aortic dissection within 30 days, and the operation was performed because of a major complication of the dissection. Four patients survived 8 to 84 months after the operation. Thus early operative intervention (before the appearance of complications) appears justified in patients with aortic dissection with the entrance tear in the descending thoracic aorta to prevent rupture of the false channel acutely or after initial healing; to prevent renal failure from compression of renal arteries by an aneurysmal false channel; to prevent true channel stenosis from compression by a thrombus-filled false channel; and possibly to prevent the recurrence of acute dissection.
本文描述了40例降主动脉入口处撕裂的主动脉夹层患者的临床及尸检结果。他们的死亡年龄在39岁至91岁之间(平均66岁);男性24例(60%),女性16例(40%)。33例(83%)患者有高血压病史,78%患者心脏重量增加。40例患者中,31例(78%)未接受手术干预,9例(22%)接受了主动脉夹层手术。在31例未接受手术治疗的患者中,9例(29%)生前确诊为主动脉夹层,22例(71%)在尸检时确诊。13例(42%)患者从主动脉夹层到死亡的间隔为30天或更短;9例(69%)患者死于假腔破裂,2例(15%)死于肾衰竭,2例(15%)死因不明。31例未接受手术治疗的患者中,18例(58%)从主动脉夹层到死亡的间隔超过30天。这18例患者中,11例(61%)的死亡与夹层有关(5例死于假腔破裂;3例死于夹层导致的肾衰竭;3例死于第二次急性夹层的假腔破裂),但其他7例(39%)患者的死亡与夹层无关,而是一种非致命并发症,具体而言,这7例患者中有4例出现了由充满血栓的假腔压迫导致的真腔狭窄。因此,31例未接受手术治疗的患者中只有3例(10%)没有主动脉夹层并发症。所有9例接受手术的患者在30天内均发生了主动脉夹层,手术是由于夹层的严重并发症而进行的。4例患者术后存活8至84个月。因此,对于降主动脉入口处撕裂的主动脉夹层患者,早期手术干预(在并发症出现之前)似乎是合理的,以防止假腔急性破裂或初始愈合后破裂;防止动脉瘤样假腔压迫肾动脉导致肾衰竭;防止充满血栓的假腔压迫导致真腔狭窄;并可能防止急性夹层复发。