Department of Neurosurgery, University of Maryland School of Medicine, Baltimore, Maryland, USA.
Stroke. 2010 Mar;41(3):531-7. doi: 10.1161/STROKEAHA.109.572644. Epub 2010 Jan 21.
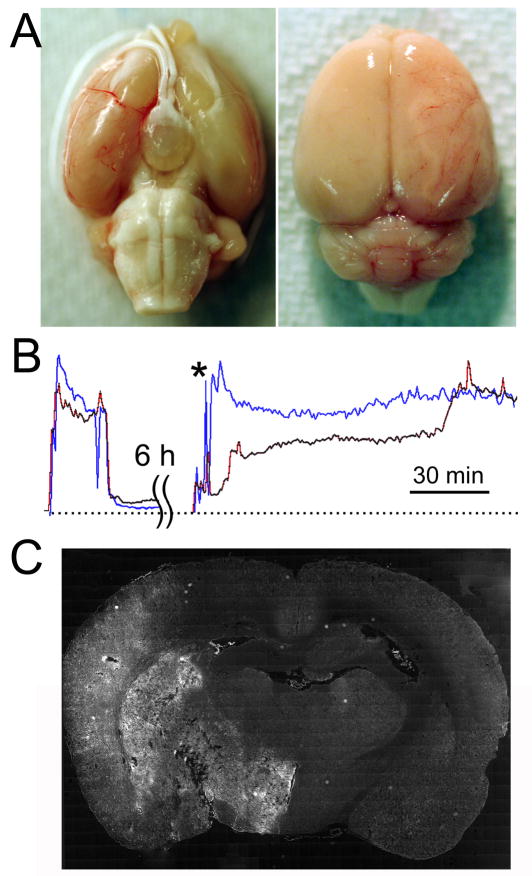
Treating patients with malignant cerebral infarctions remains a major unsolved problem in medicine. Decompressive craniectomy (DC) improves the bleak outlook but is suboptimal. Using a rat model of severe ischemia/reperfusion with very high mortality due to malignant cerebral edema, we tested the hypothesis that blocking of sulfonylurea receptor 1-regulated NC(Ca-ATP) channels with glibenclamide would compare favorably to DC when reperfusion and treatment were begun 6 hours after onset of ischemia.
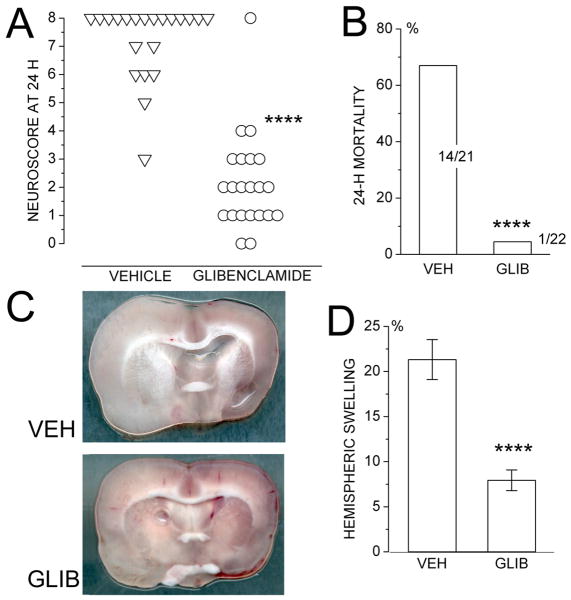
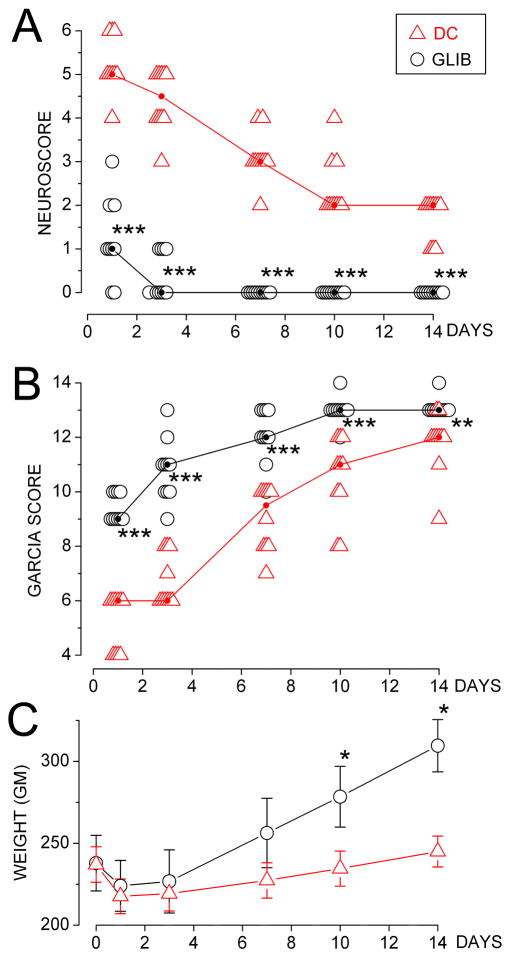
Male Wistar rats underwent filament occlusion of the middle cerebral artery to reduce laser Doppler flowmetry perfusion signals by >75%, with filament removal plus treatment 6 hours later. In rats treated with vehicle versus glibenclamide (10 microg/kg IP plus 200 ng/h SC), we compared mortality, neurologic function, and brain swelling at 24 hours. In rats treated with DC versus glibenclamide, we compared neurologic function for 2 weeks and histologic outcomes.
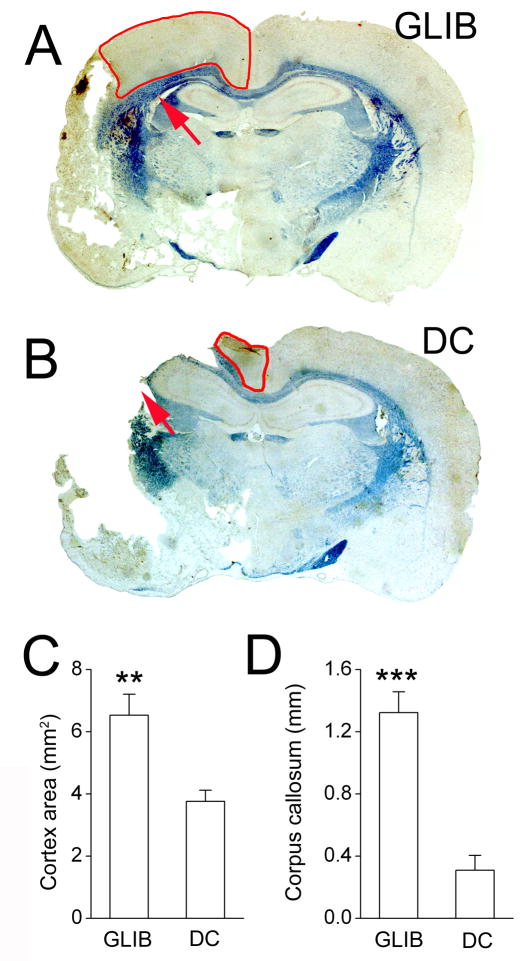
Compared with vehicle, glibenclamide treatment reduced 24-hour mortality from 67% to 5% and reduced hemispheric swelling at 24 hours from 21% to 8%. DC eliminated 24-hour mortality, but neurologic function during the next 2 weeks was significantly better with glibenclamide compared with DC. Watershed cortex and deep white matter were significantly better preserved with glibenclamide compared with DC.
In a rat model of severe ischemia/reperfusion, with reperfusion and treatment beginning 6 hours after onset of ischemia, glibenclamide is as effective as DC in preventing death from malignant cerebral edema but is superior to DC in preserving neurologic function and the integrity of watershed cortex and deep white matter.
治疗恶性脑梗死患者仍然是医学上尚未解决的主要问题。去骨瓣减压术(DC)改善了预后,但并不理想。我们使用一种因恶性脑水肿导致死亡率极高的严重缺血/再灌注大鼠模型,检验了以下假说:在缺血后 6 小时开始再灌注和治疗时,用格列本脲阻断磺酰脲受体 1 调节的 NC(Ca-ATP)通道,其效果是否优于 DC。
雄性 Wistar 大鼠进行大脑中动脉线栓阻塞,使激光多普勒血流仪灌注信号降低>75%,随后去除线栓并在 6 小时后进行治疗。在给予载体或格列本脲(10μg/kg 腹腔内注射加 200ng/h 皮下注射)的大鼠中,我们比较了 24 小时时的死亡率、神经功能和脑水肿。在给予 DC 或格列本脲的大鼠中,我们比较了 2 周时的神经功能和组织学结果。
与载体相比,格列本脲治疗将 24 小时死亡率从 67%降低至 5%,将 24 小时半球肿胀从 21%降低至 8%。DC 消除了 24 小时死亡率,但在接下来的 2 周内,格列本脲的神经功能明显优于 DC。与 DC 相比,格列本脲可显著更好地保留分水岭皮质和深部白质。
在严重缺血/再灌注大鼠模型中,再灌注和治疗开始于缺血后 6 小时,格列本脲在预防恶性脑水肿导致的死亡方面与 DC 一样有效,但在保护神经功能和保留分水岭皮质和深部白质方面优于 DC。