Division of Endocrinology, Department of Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL 60611, USA.
Transplantation. 2010 Jan 27;89(2):222-6. doi: 10.1097/TP.0b013e3181c3c2ff.
Intensive glycemic control has been shown to positively impact outcomes in an intensive care setting. Whether this practice is beneficial after liver transplantation (LT) is not known.
A retrospective review of patients undergoing LT from February 2002 to July 2007 was conducted to analyze the association between perioperative hyperglycemia and outcomes after LT. Covariates included preexisting diabetes, mean glucose 3 months pre-LT, need for insulin drip post-LT, mean total glucose during the post-LT hospitalization, age, sex, type of transplant, and model for end-stage liver disease score. Outcomes within 1 year of LT included rejection, infection, rehospitalization, prolonged ventilation, and patient/graft survival.
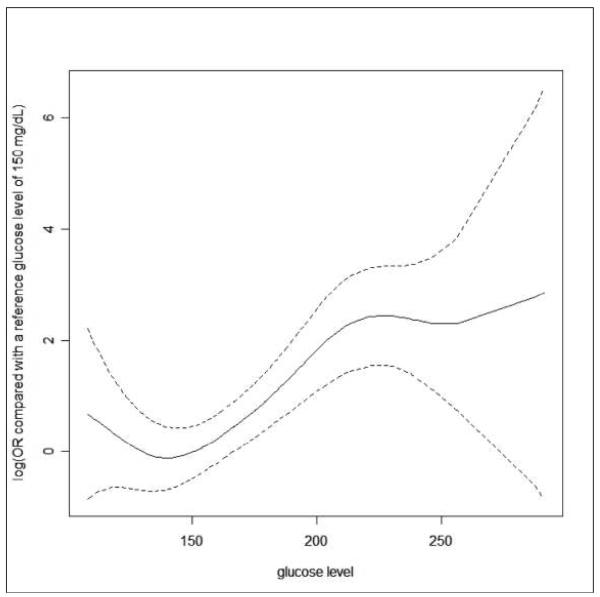
One hundred thirteen LT and 31 liver-kidney recipients were included. By multivariate logistic regression adjusting for covariates, the rejection rate was significantly lower for patients with postoperative glucose levels less than 200 mg/dL (n=114) vs. more than 200 mg/dL (n=30) (odds ratio: 0.055; 95% confidence interval: 0.0154-0.200; P<0.001). The need for prolonged ventilation was more common in patients with glucose less than 200 vs. more than 200 mg/dL (odds ratio: 4.30; 95% confidence interval: 1.284-14.388; P=0.018). Although other outcomes, infection, rehospitalization, patient/graft survival, were not different among the glucose control groups, rejection was associated with increased rehospitalizations and infections.
Our data demonstrate an association between the immediate posttransplant glycemic control and the development of subsequent rejection. Prospective trials investigating the effects of perioperative glycemic control on outcomes and morbidity after LT are warranted.
强化血糖控制已被证明可对重症监护环境中的结果产生积极影响。但这种做法在肝移植(LT)后是否有益尚不清楚。
对 2002 年 2 月至 2007 年 7 月期间接受 LT 的患者进行回顾性分析,以分析 LT 后围手术期高血糖与结局之间的关系。协变量包括:术前糖尿病、LT 前 3 个月的平均血糖、LT 后胰岛素滴注的需要、LT 后住院期间的平均总血糖、年龄、性别、移植类型和终末期肝病模型评分。LT 后 1 年内的结果包括排斥反应、感染、再住院、延长通气和患者/移植物存活率。
共纳入 113 例 LT 和 31 例肝-肾联合移植受者。通过调整协变量的多变量逻辑回归,术后血糖水平<200mg/dL(n=114)的患者排斥反应发生率明显低于血糖水平>200mg/dL(n=30)的患者(比值比:0.055;95%置信区间:0.0154-0.200;P<0.001)。血糖<200mg/dL 与血糖>200mg/dL 的患者相比,需要长时间通气的情况更为常见(比值比:4.30;95%置信区间:1.284-14.388;P=0.018)。尽管血糖控制组之间的其他结果(感染、再住院、患者/移植物存活率)没有差异,但排斥反应与再住院和感染的增加有关。
我们的数据表明,LT 后即刻血糖控制与随后排斥反应的发展之间存在关联。需要进行前瞻性试验,以调查围手术期血糖控制对 LT 后结局和发病率的影响。