Richmond Scott R, Carper Michael J, Lei Xiaoyong, Zhang Sheng, Yarasheski Kevin E, Ramanadham Sasanka
Department of Internal Medicine, Division of Endocrinology, Metabolism, and Lipid Research, Washington University School of Medicine, St. Louis, MO 63110, USA.
Biochim Biophys Acta. 2010 May;1801(5):559-66. doi: 10.1016/j.bbalip.2010.01.007. Epub 2010 Feb 1.
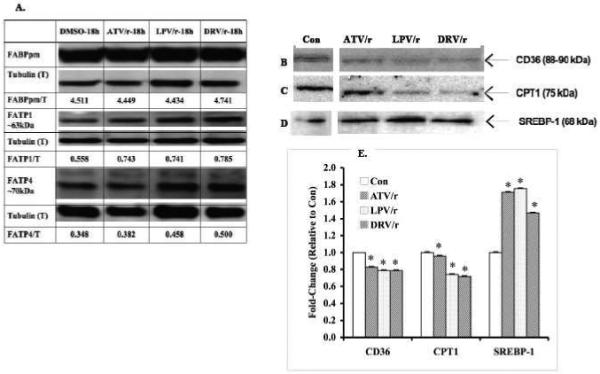
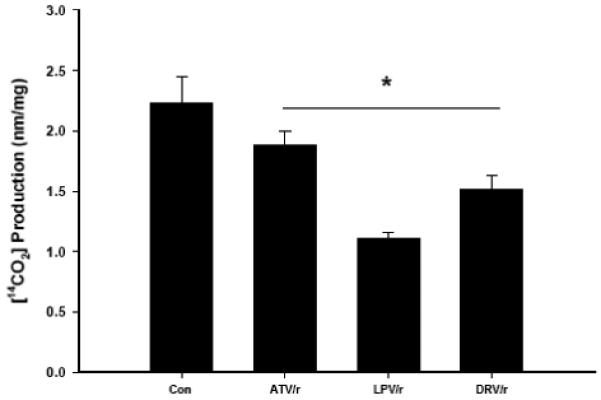
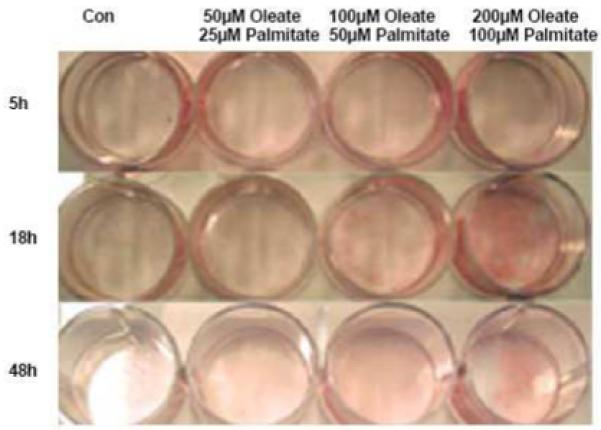
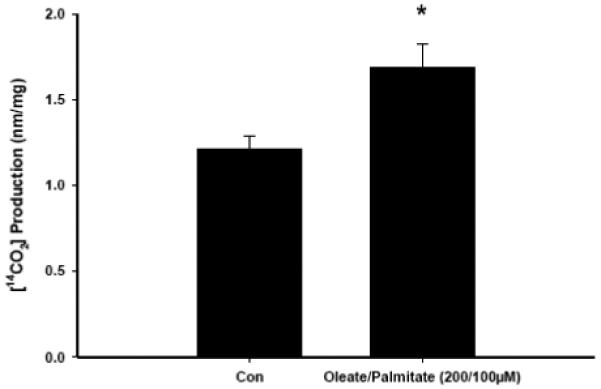
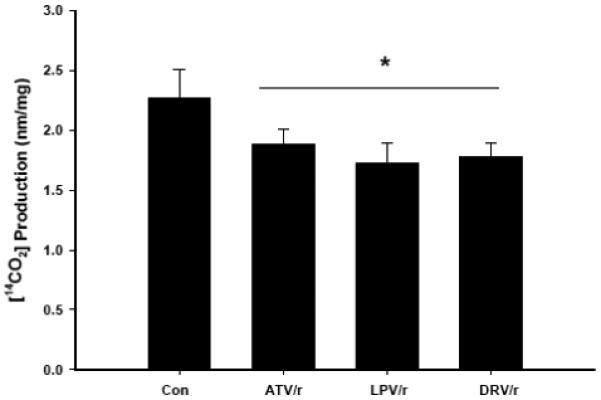
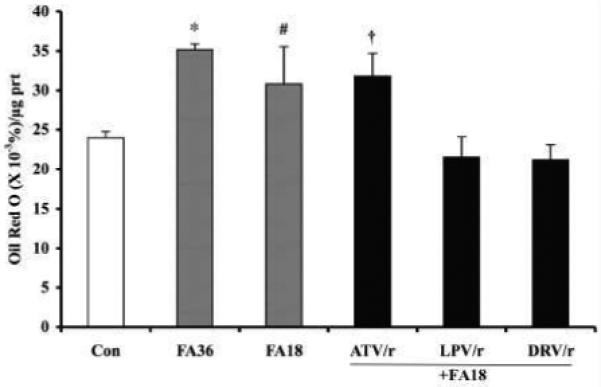
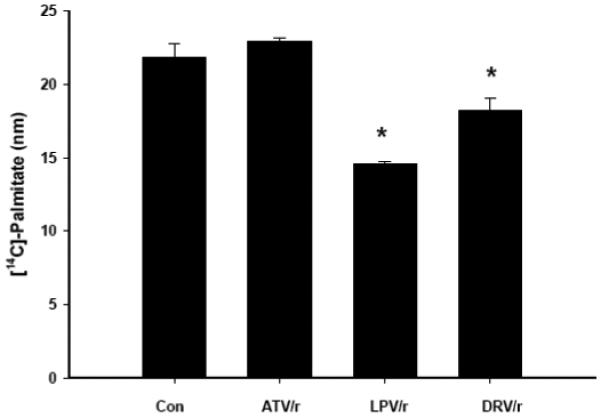
Infection with human immunodeficiency virus (HIV) and treatment with HIV-protease inhibitor (PI)-based highly active antiretroviral therapies (HAART) is associated with dysregulated fatty acid and lipid metabolism. Enhanced lipolysis, increased circulating fatty acid levels, and hepatic and intramuscular lipid accumulation appear to contribute to insulin resistance in HIV-infected people treated with PI-based HAART. However, it is unclear whether currently prescribed HIV-PIs directly alter skeletal muscle fatty acid transport, oxidation, and storage. We find that ritonavir (r, 5micromol/l) plus 20micromol/l of atazanavir (ATV), lopinavir (LPV), or darunavir (DRV) reduce palmitate oxidation(16-21%) in differentiated C2C12 myotubes. Palmitate oxidation was increased following exposure to high fatty acid media but this effect was blunted when myotubes were pre-exposed to the HIV-PIs. However, LPV/r and DRV/r, but not ATV/r suppressed palmitate uptake into myotubes. We found no effect of the HIV-PIs on FATP1, FATP4, or FABPpm but both CD36/FAT and carnitine palmitoyltransferase 1 (CPT1) were reduced by all three regimens though ATV/r caused only a small decrease in CPT1, relative to LPV/r or DRV/r. In contrast, sterol regulatory element binding protein-1 was increased by all 3 HIV-PIs. These findings suggest that HIV-PIs suppress fatty acid oxidation in murine skeletal muscle cells and that this may be related to decreases in cytosolic- and mitochondrial-associated fatty acid transporters. HIV-PIs may also directly impair fatty acid handling and partitioning in skeletal muscle, and this may contribute to the cluster of metabolic complications that occur in people living with HIV.
感染人类免疫缺陷病毒(HIV)并接受基于HIV蛋白酶抑制剂(PI)的高效抗逆转录病毒疗法(HAART)治疗与脂肪酸和脂质代谢失调有关。脂肪分解增强、循环脂肪酸水平升高以及肝脏和肌肉内脂质蓄积似乎导致接受基于PI的HAART治疗的HIV感染者出现胰岛素抵抗。然而,目前开具的HIV-PIs是否直接改变骨骼肌脂肪酸转运、氧化和储存尚不清楚。我们发现,利托那韦(r,5微摩尔/升)加20微摩尔/升的阿扎那韦(ATV)、洛匹那韦(LPV)或达芦那韦(DRV)可降低分化的C2C12肌管中的棕榈酸氧化(16 - 21%)。暴露于高脂肪酸培养基后棕榈酸氧化增加,但当肌管预先暴露于HIV-PIs时,这种作用减弱。然而,LPV/r和DRV/r,而非ATV/r抑制棕榈酸摄取到肌管中。我们发现HIV-PIs对FATP1、FATP4或FABPpm没有影响,但所有三种方案均降低了CD36/FAT和肉碱棕榈酰转移酶1(CPT1),尽管相对于LPV/r或DRV/r,ATV/r仅使CPT1略有下降。相比之下,所有三种HIV-PIs均使固醇调节元件结合蛋白-1增加。这些发现表明,HIV-PIs抑制小鼠骨骼肌细胞中的脂肪酸氧化,这可能与胞质和线粒体相关脂肪酸转运蛋白的减少有关。HIV-PIs还可能直接损害骨骼肌中的脂肪酸处理和分配,这可能导致HIV感染者出现一系列代谢并发症。