Department of Medicine, Sydvestjysk Sygehus, Esbjerg, Denmark.
Scand J Trauma Resusc Emerg Med. 2010 Feb 11;18:8. doi: 10.1186/1757-7241-18-8.
Patients referred to a medical admission unit (MAU) represent a broad spectrum of disease severity. In the interest of allocating resources to those who might potentially benefit most from clinical interventions, several scoring systems have been proposed as a triaging tool.Even though most scoring systems are not meant to be used on an individual level, they can support the more inexperienced doctors and nurses in assessing the risk of deterioration of their patients.We therefore performed a systematic review on the level of evidence of literature on scoring systems developed or validated in the MAU. We hypothesized that existing scoring systems would have a low level of evidence and only few systems would have been externally validated.
We conducted a systematic search using Medline, EMBASE and the Cochrane Library, according to the PRISMA guidelines, on scoring systems developed to assess medical patients at admission.The primary endpoints were in-hospital mortality or transfer to the intensive care unit. Studies derived for only a single or few diagnoses were excluded.The ability to identify patients at risk (discriminatory power) and agreement between observed and predicted outcome (calibration) along with the method of derivation and validation (application on a new cohort) were extracted.
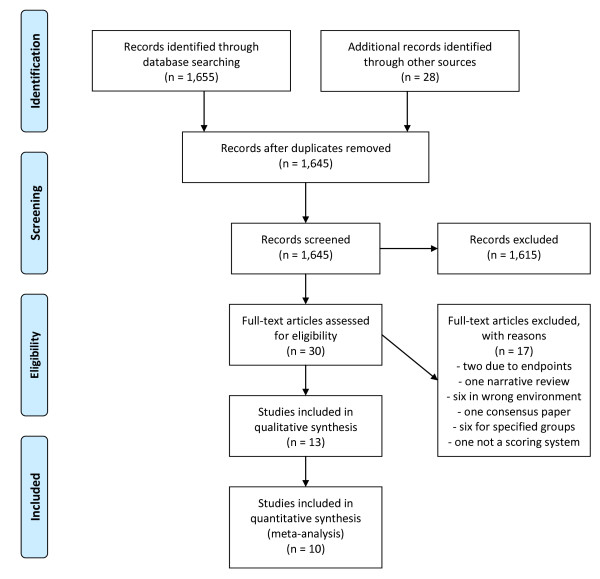
We identified 1,655 articles. Thirty were selected for further review and 10 were included in this review.Eight systems used vital signs as variables and two relied mostly on blood tests.Nine systems were derived using regression analysis and eight included patients admitted to a MAU. Six systems used in-hospital mortality as their primary endpoint.Discriminatory power was specified for eight of the scoring systems and was acceptable or better in five of these. The calibration was only specified for four scoring systems. In none of the studies impact analysis or inter-observer reliability were analyzed.None of the systems reached the highest level of evidence.
None of the 10 scoring systems presented in this article are perfect and all have their weaknesses. More research is needed before the use of scoring systems can be fully implemented to the risk assessment of acutely admitted medical patients.
被转至医疗收治单元(MAU)的患者代表了广泛的疾病严重程度。为了将资源分配给那些可能从临床干预中受益最大的患者,已经提出了几种评分系统作为分诊工具。尽管大多数评分系统并非旨在用于个体层面,但它们可以为经验不足的医生和护士提供支持,帮助他们评估患者病情恶化的风险。因此,我们对在 MAU 中开发或验证的评分系统进行了系统评价,以评估文献的证据水平。我们假设现有的评分系统证据水平较低,只有少数系统得到了外部验证。
我们按照 PRISMA 指南,使用 Medline、EMBASE 和 Cochrane Library 进行了系统搜索,以查找用于评估入院时的医疗患者的评分系统。主要终点是院内死亡率或转至重症监护病房。仅针对单一或少数诊断的研究被排除在外。我们提取了识别风险患者的能力(区分能力)、观察到的和预测结果之间的一致性(校准)以及推导和验证方法(应用于新队列)。
我们共确定了 1655 篇文章。有 30 篇文章被进一步审查,其中 10 篇被纳入本综述。有 8 个系统使用生命体征作为变量,有 2 个系统主要依赖于血液检查。有 9 个系统使用回归分析,有 8 个系统包括被收治至 MAU 的患者。有 6 个系统将院内死亡率作为主要终点。有 8 个评分系统明确了区分能力,其中 5 个系统的区分能力可接受或更好。仅有 4 个评分系统明确了校准。在这些研究中,均未分析影响分析或观察者间可靠性。没有一个系统达到了最高的证据水平。
本文介绍的 10 个评分系统没有一个是完美的,都有各自的弱点。在将评分系统完全应用于急性收治的医疗患者的风险评估之前,还需要进一步研究。