Department of Anesthesiology and Surgical Intensive Care Unit, Hôpital Bichat-Claude Bernard, Université Paris VII Denis Diderot, Assistance Publique Hôpitaux de Paris, 46 rue Henri Huchard, 75877 Paris Cedex 18, France.
Crit Care. 2010;14(1):R20. doi: 10.1186/cc8877. Epub 2010 Feb 15.
The main objective was to determine risk factors for presence of multidrug resistant bacteria (MDR) in postoperative peritonitis (PP) and optimal empirical antibiotic therapy (EA) among options proposed by Infectious Disease Society of America and the Surgical Infection Society guidelines.
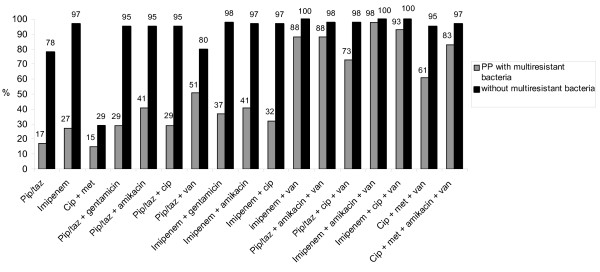
One hundred patients hospitalised in the intensive care unit (ICU) for PP were reviewed. Clinical and microbiologic data, EA and its adequacy were analysed. The in vitro activities of 9 antibiotics in relation to the cultured bacteria were assessed to propose the most adequate EA among 17 regimens in the largest number of cases.
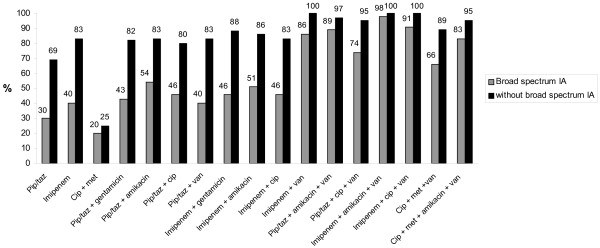
A total of 269 bacteria was cultured in 100 patients including 41 episodes with MDR. According to logistic regression analysis, the use of broad-spectrum antibiotic between initial intervention and reoperation was the only significant risk factor for emergence of MDR bacteria (odds ratio (OR) = 5.1; 95% confidence interval (CI) = 1.7 - 15; P = 0.0031). Antibiotics providing the best activity rate were imipenem/cilastatin (68%) and piperacillin/tazobactam (53%). The best adequacy for EA was obtained by combinations of imipenem/cilastatin or piperacillin/tazobactam, amikacin and a glycopeptide, with values reaching 99% and 94%, respectively. Imipenem/cilastin was the only single-drug regimen providing an adequacy superior to 80% in the absence of broad spectrum antibiotic between initial surgery and reoperation.
Interval antibiotic therapy is associated with the presence of MDR bacteria. Not all regimens proposed by Infectious Disease Society of America and the Surgical Infection Society guidelines for PP can provide an acceptable rate of adequacy. Monotherapy with imipenem/cilastin is suitable for EA only in absence of this risk factor for MDR. For other patients, only antibiotic combinations may achieve high adequacy rates.
主要目的是确定术后腹膜炎(PP)中多药耐药菌(MDR)存在的危险因素,以及美国传染病学会和外科感染学会指南提出的最佳经验性抗生素治疗(EA)。
回顾了 100 例因 PP 住院于重症监护病房(ICU)的患者。分析了临床和微生物学数据、EA 及其充分性。评估了 9 种抗生素与培养细菌的体外活性,以提出在最大数量病例中最合适的 EA 17 种方案中的 17 种方案。
共培养了 100 例患者的 269 株细菌,其中 41 例为 MDR 感染。根据逻辑回归分析,初始干预与再次手术之间使用广谱抗生素是出现 MDR 细菌的唯一显著危险因素(比值比(OR)=5.1;95%置信区间(CI)=1.7-15;P=0.0031)。提供最佳活性率的抗生素是亚胺培南/西司他丁(68%)和哌拉西林/他唑巴坦(53%)。EA 的最佳适当性通过亚胺培南/西司他丁或哌拉西林/他唑巴坦、阿米卡星和糖肽的组合获得,分别达到 99%和 94%。在初始手术和再次手术之间没有使用广谱抗生素的情况下,只有亚胺培南/西司他丁单药方案的适当性超过 80%。
间隔抗生素治疗与 MDR 细菌的存在有关。美国传染病学会和外科感染学会指南为 PP 提出的并非所有方案都能提供可接受的适当率。在没有 MDR 这种危险因素的情况下,亚胺培南/西司他丁单药治疗适用于 EA。对于其他患者,只有抗生素联合治疗才能达到高适当性率。