Pulzi Júnior Sérgio Antônio, Assunção Murillo Santucci Cesar de, Mazza Bruno Franco, Fernandes Haggéas da Silveira, Jackiu Mirian, Freitas Flávio Geraldo Resende, Machado Flávia Ribeiro
Intensive Care Sector, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Paulo, Brazil.
Sao Paulo Med J. 2009 Sep;127(5):259-65. doi: 10.1590/s1516-31802009000500003.
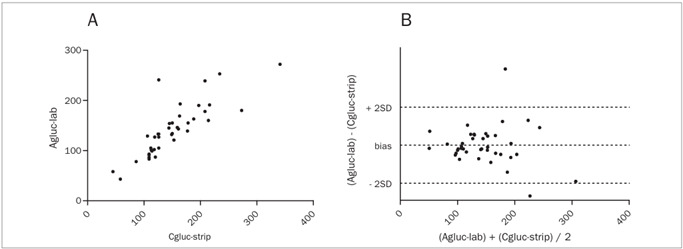
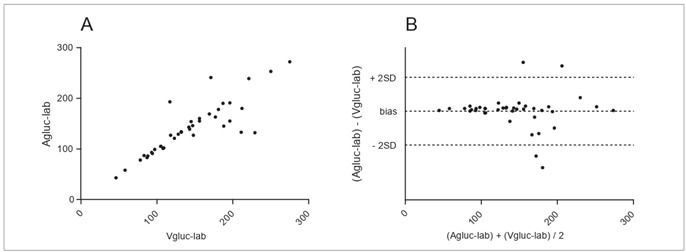
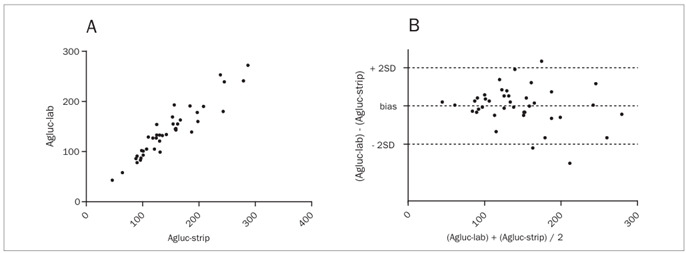
Although glucometers have not been validated for intensive care units, they are regularly used. The aim of this study was to compare and assess the accuracy and clinical agreement of arterial glucose concentration obtained using colorimetry (Agluc-lab), capillary (Cgluc-strip) and arterial (Agluc-strip) glucose concentration obtained using glucometry and central venous glucose concentration obtained using colorimetry (Vgluc-lab).
Cross-sectional study in a university hospital.
Forty patients with septic shock and stable individuals without infection were included. The correlations between measurements were assessed both in the full sample and in subgroups using noradrenalin and presenting signs of tissue hypoperfusion.
Cgluc-strip showed the poorest correlation (r = 0.8289) and agreement (-9.87 +/- 31.76). It exceeded the limits of acceptable variation of the Clinical and Laboratory Standards Institute in 23.7% of the cases, and was higher than Agluc-lab in 90% of the measurements. Agluc-strip showed the best correlation (r = 0.9406), with agreement of -6.75 +/- 19.07 and significant variation in 7.9%. For Vgluc-lab, r = 0.8549, with agreement of -4.20 +/- 28.37 and significant variation in 15.7%. Significant variation was more frequent in patients on noradrenalin (36.4% versus 6.3%; P = 0.03) but not in the subgroup with hypoperfusion. There was discordance regarding clinical management in 25%, 22% and 15% of the cases for Cgluc-strip, Vgluc-lab and Agluc-strip, respectively.
Cgluc-strip should be avoided, particularly if noradrenalin is being used. This method usually overestimates the true glucose levels and gives rise to management errors.
ACTRN12608000513314 (registered as an observational, cross-sectional study).
尽管血糖仪尚未在重症监护病房得到验证,但仍被经常使用。本研究的目的是比较和评估采用比色法测得的动脉血糖浓度(Agluc-lab)、采用血糖仪测得的毛细血管血糖浓度(Cgluc-strip)和动脉血糖浓度(Agluc-strip)以及采用比色法测得的中心静脉血糖浓度(Vgluc-lab)的准确性和临床一致性。
在一家大学医院进行的横断面研究。
纳入40例感染性休克患者和无感染的稳定个体。在全部样本以及使用去甲肾上腺素和出现组织灌注不足体征的亚组中评估测量值之间的相关性。
Cgluc-strip显示出最差的相关性(r = 0.8289)和一致性(-9.87 +/- 31.76)。在23.7%的病例中,它超出了临床和实验室标准协会可接受变异范围的限值,并且在90%的测量中高于Agluc-lab。Agluc-strip显示出最佳的相关性(r = 0.9406),一致性为-6.75 +/- 19.07,显著变异为7.9%。对于Vgluc-lab,r = 0.8549,一致性为-4.20 +/- 28.37,显著变异为15.7%。使用去甲肾上腺素的患者中显著变异更常见(36.4%对6.3%;P = 0.03),但在灌注不足亚组中并非如此。在分别有25%、22%和15%的病例中,Cgluc-strip、Vgluc-lab和Agluc-strip在临床管理方面存在不一致。
应避免使用Cgluc-strip,尤其是在使用去甲肾上腺素时。这种方法通常会高估真实血糖水平并导致管理错误。
ACTRN12608000513314(注册为一项观察性横断面研究)。