Department of Hypertension, Chair of Nephrology and Hypertension, Medical University of Lodz, Poland.
Lipids Health Dis. 2010 Feb 23;9:21. doi: 10.1186/1476-511X-9-21.
The aim of the study was to assess the influence of co-existing atrial fibrillation (AF) on inflammatory condition factors, left ventricular function, clinical course and the efficacy of statin treatment of congestive heart failure in the course of dilated cardiomyopathy (DCM).
In a prospective, randomized, open-label study, 69 patients with DCM and left ventricular ejection fraction (LVEF) < or =40% were divided into two groups, with and without AF, who were treated according to the recommended standards. 68% of patients from the group with AF and 59% of patients from the group without AF were administered atorvastatin 40 mg daily for 8 weeks and 10 mg for next 4 months. Clinical examination with the assessment of body mass index (BMI) and waist size were followed by routine laboratory tests, measurement of concentration of tumor necrosis factor (TNF-alpha), interleukin-6 (IL-6), and IL-10 in blood plasma, N-terminal pro-brain natriuretic peptide (NT-proBNP) concentration in blood serum, echocardiographic examination, and the assessment of exercise capacity in 6-minute walk test (6-MWT). After six months, morbidity rate and the number of heart failure hospitalizations were also observed.
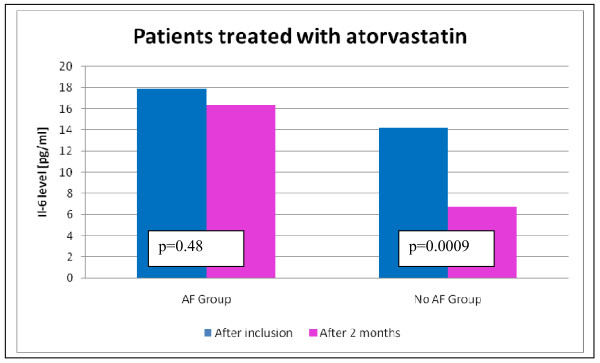
In the whole population of patients, a significantly higher concentration of NT-proBNP was observed in the AF group (2669 +/- 2192 vs 1540 +/- 1067, p = 0.02). After statin treatment, in patients with DCM and co-existing AF, higher values of NT-proBNP and IL-6 were observed compared to non-AF patients (1530 +/- 1054 vs 1006 +/- 1195, p = 0.04 and (14.16 +/- 13.40 vs 6.74 +/- 5.45, p = 0.02, respectively).
In patients with DCM and co-existing AF, a weaker effect of atorvastatin concerning the reduction of IL-6 and NT-proBNP concentration was observed than in patients without atrial fibrillation.
本研究旨在评估合并存在的心房颤动(AF)对炎症状态因子、左心室功能、临床病程以及充血性心力衰竭他汀类药物治疗疗效的影响,研究对象为扩张型心肌病(DCM)患者。
在一项前瞻性、随机、开放标签的研究中,将 69 名左心室射血分数(LVEF)≤40%的 DCM 患者分为伴有和不伴有 AF 的两组,两组均根据推荐标准进行治疗。其中,AF 组有 68%的患者和无 AF 组有 59%的患者接受阿托伐他汀 40mg 每日治疗 8 周,然后改为 10mg 每日治疗 4 个月。临床检查包括体重指数(BMI)和腰围评估,以及常规实验室检查、肿瘤坏死因子(TNF-α)、白细胞介素-6(IL-6)和白细胞介素-10(IL-10)在血浆中的浓度、血清 N 端脑钠肽前体(NT-proBNP)浓度、超声心动图检查和 6 分钟步行试验(6-MWT)运动能力评估。6 个月后,还观察了发病率和心力衰竭住院次数。
在所有患者中,AF 组的 NT-proBNP 浓度明显更高(2669+/-2192 比 1540+/-1067,p=0.02)。他汀类药物治疗后,与非 AF 患者相比,DCM 合并 AF 患者的 NT-proBNP 和 IL-6 值更高(1530+/-1054 比 1006+/-1195,p=0.04 和(14.16+/-13.40 比 6.74+/-5.45,p=0.02)。
与无房颤患者相比,DCM 合并 AF 患者使用阿托伐他汀降低 IL-6 和 NT-proBNP 浓度的效果较弱。