Public Health GIS Unit, School of Health and Related Research, University of Sheffield, Regent Court, 30 Regent Street, Sheffield S14DA, UK.
BMC Public Health. 2010 Feb 25;10:99. doi: 10.1186/1471-2458-10-99.
Many causes of death are directly attributable to the toxic effects of alcohol and deaths from these causes are increasing in the United Kingdom. The aim of this study was to investigate variation in alcohol-related mortality in relation to socioeconomic deprivation, urban-rural location and age within a national context.
An ecological study design was used with data from 8797 standard table wards in England and Wales. The methodology included using the Carstairs Index as a measure of socioeconomic deprivation at the small-area level and the national harmonised classification system for urban and rural areas in England and Wales. Alcohol-related mortality was defined using the National Statistics definition, devised for tracking national trends in alcohol-related deaths. Deaths from liver cirrhosis accounted for 85% of all deaths included in this definition. Deaths from 1999-2003 were examined and 2001 census ward population estimates were used as the denominators.
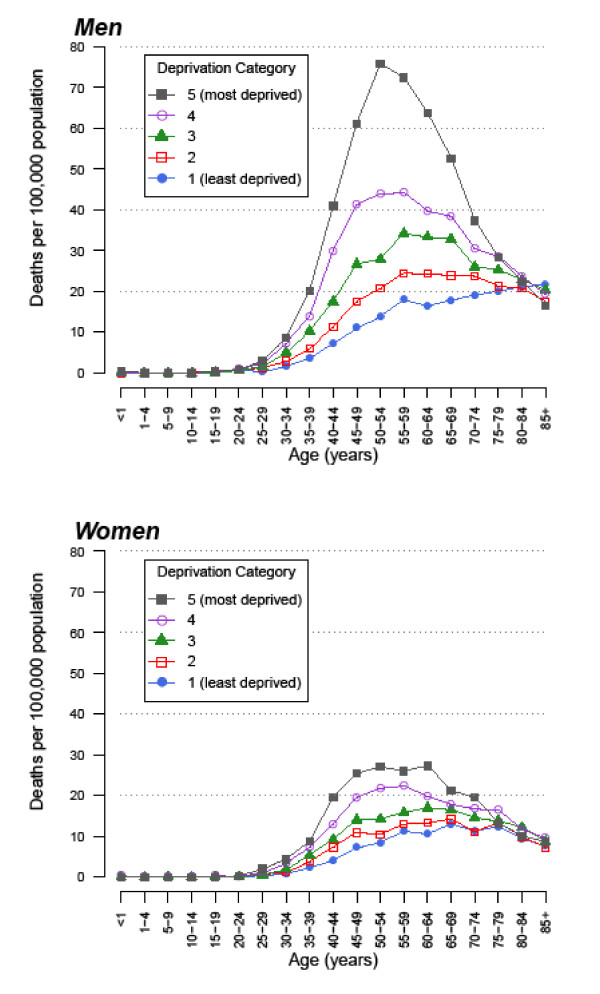
The analysis was based on 28,839 deaths. Alcohol-related mortality rates were higher in men and increased with increasing age, generally reaching peak levels in middle-aged adults. The 45-64 year age group contained a quarter of the total population but accounted for half of all alcohol-related deaths. There was a clear association between alcohol-related mortality and socioeconomic deprivation, with progressively higher rates in more deprived areas. The strength of the association varied with age. Greatest relative inequalities were seen amongst people aged 25-44 years, with relative risks of 4.73 (95% CI 4.00 to 5.59) and 4.24 (95% CI 3.50 to 5.13) for men and women respectively in the most relative to the least deprived quintiles. People living in urban areas experienced higher alcohol-related mortality relative to those living in rural areas, with differences remaining after adjustment for socioeconomic deprivation. Adjusted relative risks for urban relative to rural areas were 1.35 (95% CI 1.20 to 1.52) and 1.13 (95% CI 1.01 to 1.25) for men and women respectively.
Large inequalities in alcohol-related mortality exist between sub-groups of the population in England and Wales. These should be considered when designing public health policies to reduce alcohol-related harm.
许多死亡原因直接归因于酒精的毒性作用,而英国因这些原因导致的死亡人数正在增加。本研究的目的是在全国范围内调查与社会经济贫困程度、城乡位置和年龄有关的酒精相关死亡率的变化。
本研究采用生态研究设计,使用英格兰和威尔士 8797 个标准表区的数据。该方法包括使用 Carstairs 指数作为小区域社会经济贫困程度的衡量标准,以及英格兰和威尔士城乡统一分类系统。使用国家统计局定义的酒精相关死亡率,用于跟踪全国范围内与酒精相关的死亡趋势。本定义中包括的所有死亡人数中,有 85%死于肝硬化。对 1999-2003 年的死亡情况进行了检查,并使用 2001 年人口普查区的人口估计数作为分母。
本分析基于 28839 例死亡。男性的酒精相关死亡率较高,且随年龄增长而增加,通常在中年人群中达到峰值。45-64 岁年龄组占总人口的四分之一,但占所有酒精相关死亡人数的一半。酒精相关死亡率与社会经济贫困程度之间存在明显关联,贫困程度越高的地区死亡率越高。这种关联的强度随年龄而变化。在 25-44 岁人群中,相对风险最高,最贫困五分位数与最不贫困五分位数相比,男性和女性的相对风险分别为 4.73(95%CI 4.00 至 5.59)和 4.24(95%CI 3.50 至 5.13)。与居住在农村地区的人相比,居住在城市地区的人酒精相关死亡率更高,在调整社会经济贫困程度后,差异仍然存在。与农村地区相比,城市地区的调整后男性和女性的相对风险分别为 1.35(95%CI 1.20 至 1.52)和 1.13(95%CI 1.01 至 1.25)。
英格兰和威尔士人口的亚组之间存在与酒精相关的死亡率的巨大不平等。在制定减少酒精相关危害的公共卫生政策时,应考虑到这些不平等。