Department of Anesthesiology and Perioperative Medicine, The University of Texas M.D. Anderson Cancer Center, Houston, USA.
Br J Anaesth. 2010 Apr;104(4):465-71. doi: 10.1093/bja/aeq034. Epub 2010 Feb 26.
This pilot study compared the risk predictive value of preoperative physiological capacity (PC: defined by gas exchange measured during cardiopulmonary exercise testing) with the ASA physical status classification in the same patients (n=32) undergoing major abdominal cancer surgery.
Uni- and multivariate logistic regression models were fitted to measurements of PC and ASA rank data determining their predictive value for postoperative morbidity. Receiver operating characteristic (ROC) curves were used to discriminate between the predictive abilities, exploring trade-offs between sensitivity and specificity.
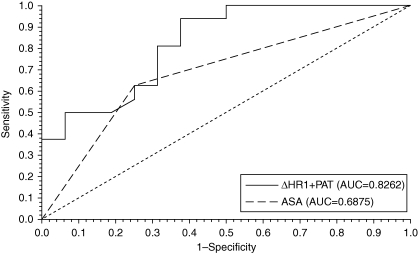
Individual statistically significant predictors of postoperative morbidity included the ASA rank [P=0.038, area under the curve (AUC)=0.688, sensitivity=0.630, specificity=0.750] and three newly identified measures of PC: PAT (% predicted anaerobic threshold achieved, <75% vs > or =75%), DeltaHR1 (heart rate response from rest to the anaerobic threshold), and HR3 (heart rate at the anaerobic threshold). A two-variable model of PC measurements (DeltaHR1+PAT) was also shown to be statistically significant in the prediction of postoperative morbidity (P=0.023, AUC=0.826, sensitivity=0.813, specificity=0.688).
Three newly identified PC measures and the ASA rank were significantly associated with postoperative morbidity; none showed a statistically greater association compared with the others. PC appeared to improve predictive sensitivity. The potential for new unidentified measures of PC to predict postoperative outcomes remains unexplored.
本初步研究比较了术前生理能力(PC:通过心肺运动试验测量得出的气体交换定义)与同一接受大型腹部癌症手术的患者的美国麻醉医师协会(ASA)身体状况分级(n=32)的风险预测价值。
采用单变量和多变量逻辑回归模型拟合 PC 和 ASA 等级数据的测量值,确定它们对术后发病率的预测价值。使用接收者操作特征(ROC)曲线来区分预测能力,探索敏感性和特异性之间的权衡。
个体术后发病率的统计学显著预测因子包括 ASA 等级 [P=0.038,曲线下面积(AUC)=0.688,敏感性=0.630,特异性=0.750]和三个新确定的 PC 指标:PAT(%预测无氧阈达到,<75%与≥75%)、DeltaHR1(从休息到无氧阈的心率反应)和 HR3(无氧阈时的心率)。PC 测量的两变量模型(DeltaHR1+PAT)也被证明在预测术后发病率方面具有统计学意义(P=0.023,AUC=0.826,敏感性=0.813,特异性=0.688)。
三个新确定的 PC 指标和 ASA 等级与术后发病率显著相关;与其他指标相比,均未显示出统计学上更大的关联。PC 似乎提高了预测的敏感性。PC 预测术后结果的新未识别指标的潜力仍有待探索。