Department of Radiation Oncology, Ludwig-Maximilians-University München, Marchioninistr, 15, 81377 München, Germany.
Radiat Oncol. 2010 Mar 18;5:23. doi: 10.1186/1748-717X-5-23.
Several randomized trials have documented the value of radiation dose escalation in patients with prostate cancer, especially in patients with intermediate risk profile. Up to now dose escalation is usually applied to the whole prostate. IMRT and related techniques currently allow for dose escalation in sub-volumes of the organ. However, the sensitivity of the imaging modality and the fact that small islands of cancer are often dispersed within the whole organ may limit these approaches with regard to a clear clinical benefit. In order to assess potential effects of a dose escalation in certain sub-volumes based on choline PET imaging a mathematical dose-response model was developed.
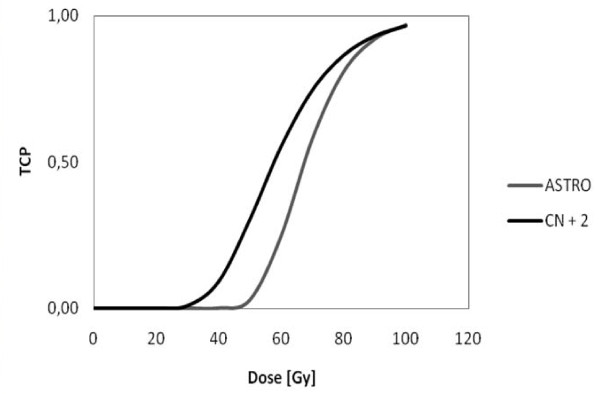
Based on different assumptions for alpha/beta, gamma 50, sensitivity and specificity of choline PET, the influence of the whole prostate and simultaneous integrated boost (SIB) dose on tumor control probability (TCP) was calculated. Based on the given heterogeneity of all potential variables certain representative permutations of the parameters were chosen and, subsequently, the influence on TCP was assessed.
Using schedules with 74 Gy within the whole prostate and a SIB dose of 90 Gy the TCP increase ranged from 23.1% (high detection rate of choline PET, low whole prostate dose, high gamma 50/ASTRO definition for tumor control) to 1.4% TCP gain (low sensitivity of PET, high whole prostate dose, CN + 2 definition for tumor control) or even 0% in selected cases. The corresponding initial TCP values without integrated boost ranged from 67.3% to 100%. According to a large data set of intermediate-risk prostate cancer patients the resulting TCP gains ranged from 22.2% to 10.1% (ASTRO definition) or from 13.2% to 6.0% (CN + 2 definition).
Although a simplified mathematical model was employed, the presented model allows for an estimation in how far given schedules are relevant for clinical practice. However, the benefit of a SIB based on choline PET seems less than intuitively expected. Only under the assumption of high detection rates and low initial TCP values the TCP gain has been shown to be relevant.
Based on the employed assumptions, specific dose escalation to choline PET positive areas within the prostate may increase the local control rates. Due to the lack of exact PET sensitivity and prostate alpha/beta parameter, no firm conclusions can be made. Small variations may completely abrogate the clinical benefit of a SIB based on choline PET imaging.
多项随机试验已经证实,提高前列腺癌患者的放射剂量具有重要价值,尤其是对中危患者而言。目前,提高剂量的方法通常应用于整个前列腺。调强放疗和相关技术目前可以对器官的亚体积进行剂量升级。然而,由于成像方式的敏感性以及癌症的小病灶常常分散在整个器官中,这些方法可能无法带来明显的临床获益。为了评估基于胆碱 PET 成像的特定亚体积剂量升级的潜在效果,开发了一种剂量-反应数学模型。
根据不同的α/β、γ 50、胆碱 PET 的敏感性和特异性假设,计算了整个前列腺和同时整合升压(SIB)剂量对肿瘤控制概率(TCP)的影响。基于所有潜在变量的给定异质性,选择了某些代表性的参数排列,并随后评估了对 TCP 的影响。
使用 74 Gy 的全前列腺剂量和 90 Gy 的 SIB 剂量的方案,TCP 的增加幅度从 23.1%(胆碱 PET 高检测率、低全前列腺剂量、ASTRO 肿瘤控制定义的高γ 50/ASTRO)到 1.4% TCP 增益(PET 低敏感性、高全前列腺剂量、肿瘤控制的 CN + 2 定义),甚至在某些情况下为 0%。没有整合升压的初始 TCP 值从 67.3%到 100%不等。根据中危前列腺癌患者的大型数据集,所得的 TCP 增益从 22.2%到 10.1%(ASTRO 定义)或从 13.2%到 6.0%(CN + 2 定义)不等。
尽管采用了简化的数学模型,但所提出的模型允许对特定方案在多大程度上与临床实践相关进行估计。然而,基于胆碱 PET 的 SIB 的获益似乎并不像直观预期的那样大。只有在高检测率和低初始 TCP 值的假设下,TCP 增益才具有相关性。
根据所采用的假设,对前列腺内胆碱 PET 阳性区域进行特定的剂量升级可能会提高局部控制率。由于缺乏确切的 PET 敏感性和前列腺α/β 参数,因此无法得出明确的结论。微小的变化可能会完全消除基于胆碱 PET 成像的 SIB 的临床获益。