Department of Public and Occupational Health, EMGO Institute for Health and Care Research, VU University Medical Centre, Amsterdam, The Netherlands.
BMC Musculoskelet Disord. 2010 Mar 28;11:60. doi: 10.1186/1471-2474-11-60.
Within the working population there is a vulnerable group: workers without an employment contract and workers with a flexible labour market arrangement, e.g. temporary agency workers. In most cases, when sick-listed, these workers have no workplace/employer to return to. Also, for these workers access to occupational health care is limited or even absent in many countries. For this vulnerable working population there is a need for tailor-made occupational health care, including the presence of an actual return-to-work perspective. Therefore, a participatory return-to-work program has been developed based on a successful return-to-work intervention for workers, sick-listed due to low back pain.The objective of this paper is to describe the design of a randomised controlled trial to study the (cost-)effectiveness of this newly developed participatory return-to-work program adapted for temporary agency workers and unemployed workers, sick-listed due to musculoskeletal disorders, compared to usual care.
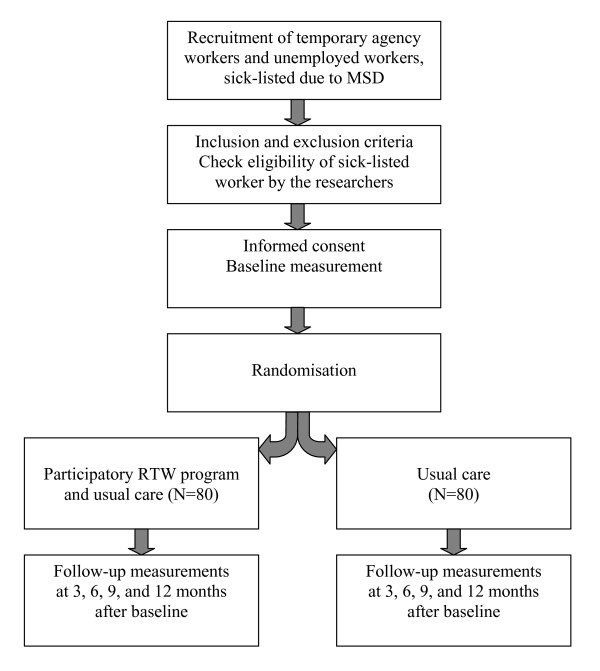
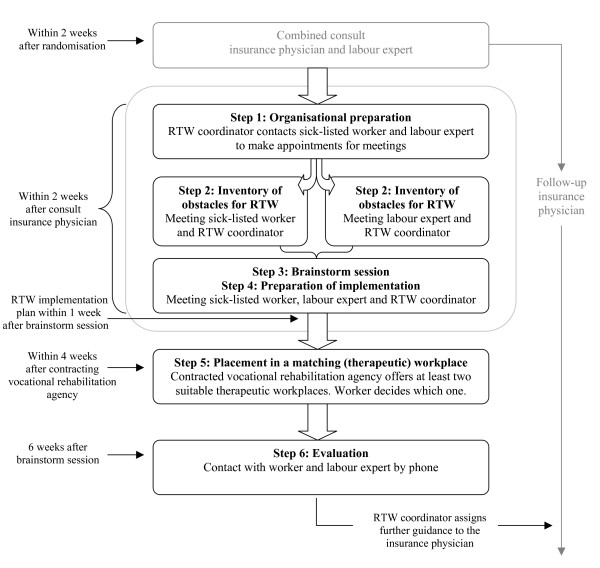
METHODS/DESIGN: The design of this study is a randomised controlled trial with one year of follow-up. The study population consists of temporary agency workers and unemployed workers sick-listed between 2 and 8 weeks due to musculoskeletal disorders. The new return-to-work program is a stepwise program aimed at making a consensus-based return-to-work implementation plan with the possibility of a (therapeutic) workplace to return-to-work. Outcomes are measured at baseline, 3, 6, 9 and 12 months. The primary outcome measure is duration of the sickness benefit period after the first day of reporting sick. Secondary outcome measures are: time until first return-to-work, total number of days of sickness benefit during follow-up; functional status; intensity of musculoskeletal pain; pain coping; and attitude, social influence and self-efficacy determinants. Cost-benefit is evaluated from an insurer's perspective. A process evaluation is part of this study.
For sick-listed workers without an employment contract there can be gained a lot by improving occupational health care, including return-to-work guidance, and by minimising the 'labour market handicap' by creating a return-to-work perspective. In addition, reduction of sickness absence and work disability, i.e. a reduction of disability claims, may result in substantial benefits for the Dutch Social Security System.
NTR1047.
在劳动人口中,存在一个脆弱群体:无劳动合同的工人和劳动力市场安排灵活的工人,例如临时工。在大多数情况下,这些工人一旦请病假,就会失业,无处可归。此外,在许多国家,这些工人获得职业保健的机会有限甚至不存在。对于这个脆弱的劳动群体,需要提供定制的职业保健服务,包括提供实际的重返工作岗位的前景。因此,基于一项成功的针对因下背痛而请病假的工人的重返工作岗位干预措施,开发了一种参与式重返工作岗位计划。本文的目的是描述一项随机对照试验的设计,以研究为因肌肉骨骼疾病而请病假 2 至 8 周的临时工和失业工人量身定制的这种新的参与式重返工作岗位计划的(成本)效益,与常规护理相比。
方法/设计:本研究的设计是一项为期一年随访的随机对照试验。研究人群包括因肌肉骨骼疾病而请病假 2 至 8 周的临时工和失业工人。新的重返工作岗位计划是一个分阶段的计划,旨在制定基于共识的重返工作岗位实施计划,并有可能返回(治疗性)工作场所。结果在基线、3、6、9 和 12 个月时进行测量。主要结局指标是从报告病假的第一天起病假津贴期的持续时间。次要结局指标是:首次重返工作岗位的时间、随访期间总病假天数;功能状态;肌肉骨骼疼痛强度;疼痛应对;以及态度、社会影响和自我效能决定因素。从保险公司的角度评估成本效益。该研究的一部分是进行过程评估。
对于没有劳动合同的请病假工人来说,通过改善职业保健服务,包括重返工作岗位指导,并通过创造重返工作岗位的前景来最小化“劳动力市场劣势”,可以获得很多好处。此外,减少病假和工作残疾,即减少残疾索赔,可能会给荷兰社会保障系统带来实质性的好处。
NTR1047。