Department of Obstetrics and Gynaecology, University Medical Centre Groningen, PO Box 30.001, 9700 RB, Groningen, the Netherlands.
BMC Womens Health. 2010 May 11;10:16. doi: 10.1186/1472-6874-10-16.
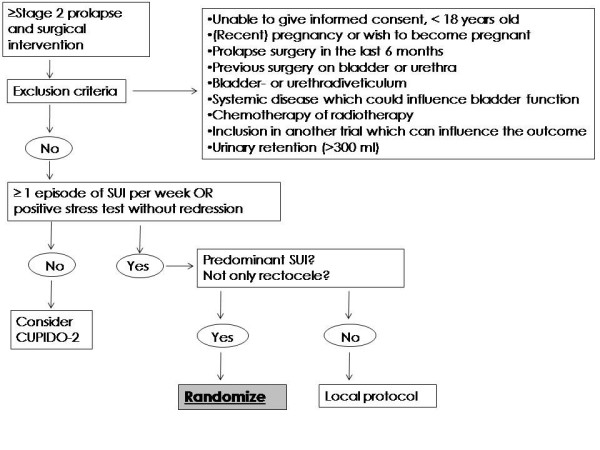
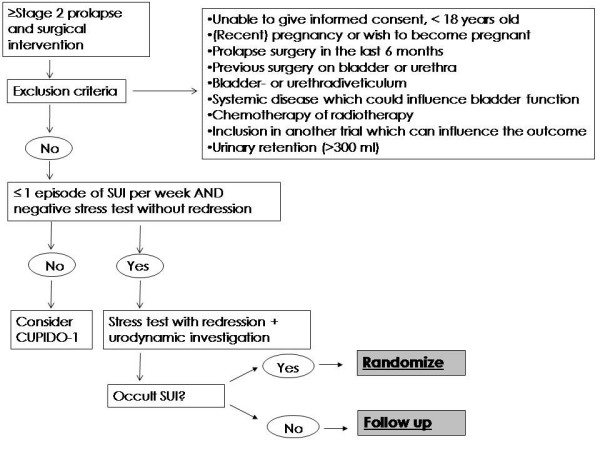
About 40% of all patients with genital prolapse report stress-incontinence. In about half of the 60% patients that do not report stress-incontinence, occult urinary stress-incontinence can be detected. In these patients stress-incontinence is masked due to kinking or compression of the urethra by the prolapse.In case surgical correction is indicated there are two strategies to manage patients with combined prolapse and (occult) stress incontinence. This strategy is either (i) a combination of prolapse surgery and stress-incontinence surgery or (ii) to correct the prolapse first and evaluate afterwards whether additional stress-incontinence surgery is indicated. The advantage of combining prolapse and stress-incontinence surgery is that only few patients report stress-incontinence following such combination. However, this combination has been associated with an increased risk on complications, of which the development of obstructive micturition symptoms, overactive bladder symptoms and bladder retention are the most important ones. Furthermore, combining two procedures may be unnecessary as performing only prolapse surgery may cure stress-incontinence. In the randomized CUPIDO trials both strategies are compared in patients with prolapse and evident stress incontinence (CUPIDO I trial) and in patients with prolapse and occult stress incontinence (CUPIDO II trial).
METHODS/DESIGN: The CUPIDO trials are two multicenter randomized controlled trials in which women with stress urinary incontinence (SUI) or occult stress urinary incontinence (OSUI) are randomized to prolapse surgery combined with anti incontinence surgery (concomitant surgery) or to prolapse surgery only. Patients with at least stage 2 POP are eligible, women with evident SUI are randomized in CUPIDO I. Patients without SUI are eligible for CUPIDO II and will have urodynamic evaluation or a standardized redression test. Women with OSUI are randomized, women without OSUI are followed up but not randomized. The primary outcome measure is absence of SUI twelve months after surgery. Furthermore, economic evaluations are conducted, and the effectiveness of urodynamic investigation is evaluated against a non-invasive way to determine SUI in women with POP. A total of 450 women will be included in the study.
Trial registration http://www.trialregister.nl NTRR 1197 en 1070.
大约 40%的生殖道脱垂患者报告存在压力性尿失禁。在不报告压力性尿失禁的 60%患者中,约有一半可以检测到隐匿性尿失禁。在这些患者中,由于脱垂导致尿道扭曲或受压,压力性尿失禁被掩盖。如果需要手术矫正,对于同时患有脱垂和(隐匿性)压力性尿失禁的患者,有两种治疗策略。该策略可以是(i)脱垂手术与压力性尿失禁手术相结合,或(ii)首先矫正脱垂,然后评估是否需要额外的压力性尿失禁手术。联合脱垂和压力性尿失禁手术的优点是只有少数患者在联合手术后报告存在压力性尿失禁。然而,这种联合治疗与并发症风险增加有关,其中最重要的是排尿障碍症状、膀胱过度活动症症状和膀胱潴留的发展。此外,联合两种手术可能是不必要的,因为仅行脱垂手术可能会治愈压力性尿失禁。在随机对照的 CUPIDO 试验中,这两种策略在同时患有脱垂和明显压力性尿失禁(CUPIDO I 试验)以及同时患有脱垂和隐匿性压力性尿失禁(CUPIDO II 试验)的患者中进行了比较。
方法/设计:CUPIDO 试验是两项多中心随机对照试验,其中患有压力性尿失禁(SUI)或隐匿性压力性尿失禁(OSUI)的女性患者被随机分为同时行脱垂手术和抗失禁手术(联合手术)或仅行脱垂手术。至少患有 2 期 POP 的女性患者符合条件,具有明显 SUI 的女性患者被随机分为 CUPIDO I 组。没有 SUI 的患者符合 CUPIDO II 组的条件,并将进行尿动力学评估或标准化复位试验。患有 OSUI 的女性患者被随机分组,没有 OSUI 的女性患者则被随访但不随机分组。主要结局指标是手术后 12 个月无 SUI。此外,还进行了经济评估,并评估了尿动力学检查对女性 POP 患者非侵入性确定 SUI 的有效性。共有 450 名女性将参与该研究。
试验注册网址 http://www.trialregister.nl NTRR 1197 和 1070。