Washington University School of Medicine, St. Louis, MO 63110-1093, USA.
Acta Neuropathol. 2010 Aug;120(2):237-52. doi: 10.1007/s00401-010-0695-9. Epub 2010 May 13.
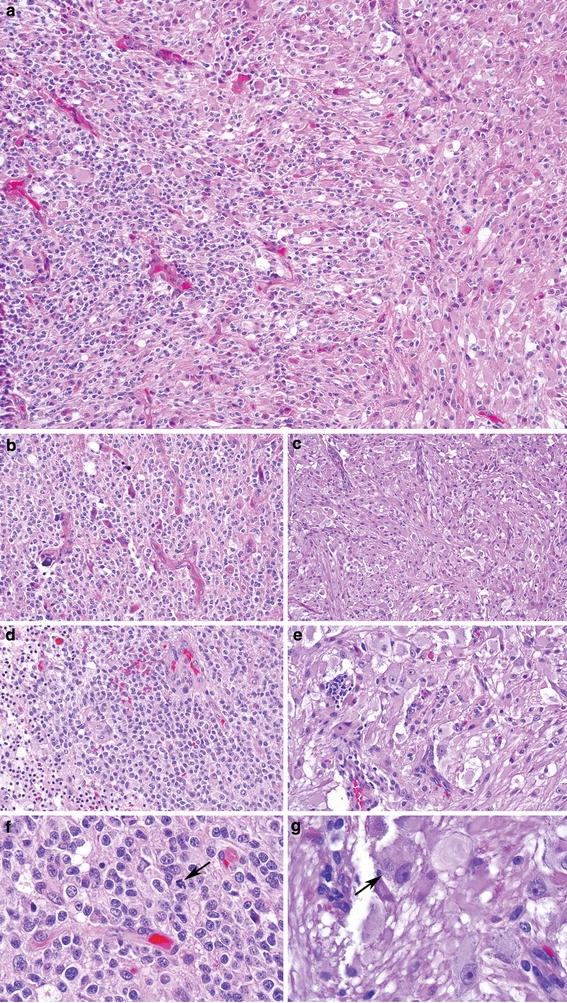
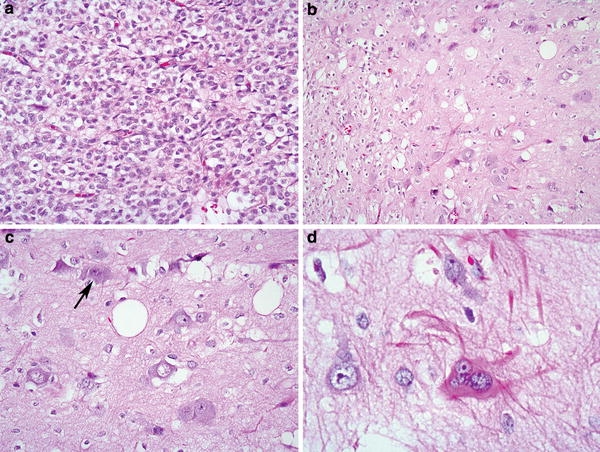
Although oligodendroglial neoplasms are traditionally considered purely glial, increasing evidence suggests that they are capable of neuronal or neurocytic differentiation. Nevertheless, ganglioglioma-like foci (GGLF) have not been previously described. Herein, we report seven examples where the primary differential diagnosis was a ganglioglioma with an oligodendroglial component. These five male and two female patients ranged in age from 29 to 63 (median 44) years at initial presentation and neuroimaging features were those of diffuse gliomas in general. At presentation, the glial component was oligodendroglioma in six and oligoastrocytoma in one; one was low-grade and six were anaplastic. A sharp demarcation from adjacent GGLF was common, although some intermingling was always present. The GGLF included enlarged dysmorphic and occasionally binucleate ganglion cells, Nissl substance, expression of neuronal antigens, GFAP-positive astrocytic elements, and low Ki-67 labeling indices. In contrast to classic ganglioglioma, however, cases lacked eosinophilic granular bodies and CD34-positive tumor cells. Scattered bizarre astrocytes were also common and one case had focal neurocytic differentiation. By FISH analysis, five cases showed 1p/19q codeletion. In the four cases with deletions and ample dysmorphic ganglion cells for analysis, the deletions were found in both components. At last follow-up, two patients suffered recurrences, one developed radiation necrosis mimicking recurrence, and one died of disease 7.5 years after initial surgery. We conclude that GGLF represents yet another form of neuronal differentiation in oligodendroglial neoplasms. Recognition of this pattern will prevent a misdiagnosis of ganglioglioma with its potential for under-treatment.
尽管少突胶质细胞瘤传统上被认为是纯粹的神经胶质肿瘤,但越来越多的证据表明它们具有神经元或神经细胞分化的能力。然而,神经节胶质细胞瘤样病灶(ganglioglioma-like foci,GGLF)以前并未被描述过。在此,我们报告了 7 例最初的鉴别诊断为具有少突胶质成分的神经节胶质细胞瘤的病例。这 5 例男性和 2 例女性患者的初诊年龄为 29 至 63 岁(中位数为 44 岁),神经影像学特征通常为弥漫性胶质瘤。初诊时,胶质成分在 6 例中为少突胶质细胞瘤,1 例为少突星形细胞瘤;1 例为低级别,6 例为间变性。与相邻 GGLF 的明显分界很常见,尽管总是存在一些混合。GGLF 包括增大的畸形和偶尔双核的神经节细胞、尼氏体、神经元抗原的表达、GFAP 阳性的星形细胞成分以及低的 Ki-67 标记指数。然而,与经典的神经节胶质细胞瘤不同,这些病例缺乏嗜酸性颗粒体和 CD34 阳性的肿瘤细胞。散在的奇异星形细胞瘤也很常见,有 1 例有局灶性神经细胞分化。通过 FISH 分析,5 例显示 1p/19q 缺失。在 4 例有缺失且有足够数量的畸形神经节细胞进行分析的病例中,缺失均存在于两个成分中。在最后一次随访中,2 例患者复发,1 例发生放射性坏死,类似于复发,1 例患者在初始手术后 7.5 年因疾病死亡。我们得出结论,GGLF 代表了少突胶质细胞瘤中另一种神经元分化形式。认识到这种模式将防止误诊为神经节胶质细胞瘤,从而避免潜在的治疗不足。