Institute for Prevention of Cardiovascular Diseases, University of Munich, Munich, Germany.
Current Address: 1st Department of Medicine, University of Pécs, Pécs, Hungary.
Thromb J. 2010 May 13;8:9. doi: 10.1186/1477-9560-8-9.
Poor platelet inhibition by aspirin or clopidogrel has been associated with adverse outcomes in patients with cardiovascular diseases. A reliable and facile assay to measure platelet inhibition after treatment with aspirin and a P2Y12 antagonist is lacking. Multiple electrode aggregometry (MEA), which is being increasingly used in clinical studies, is sensitive to platelet inhibition by aspirin and clopidogrel, but a critical evaluation of MEA monitoring of dual anti-platelet therapy with aspirin and P2Y12 antagonists is missing.
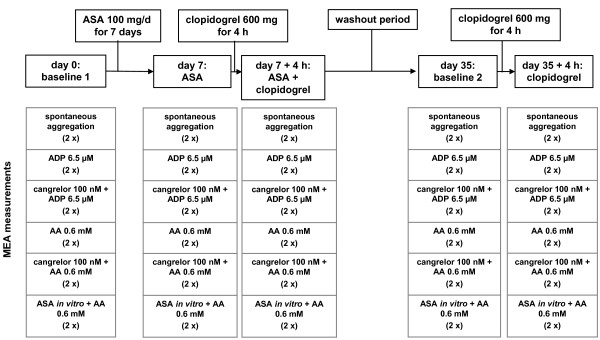
By performing in vitro and ex vivo experiments, we evaluated in healthy subjects the feasibility of using MEA to monitor platelet inhibition of P2Y12 antagonists (clopidogrel in vivo, cangrelor in vitro) and aspirin (100 mg per day in vivo, and 1 mM or 5.4 mM in vitro) alone, and in combination. Statistical analyses were performed by the Mann-Whitney rank sum test, student' t-test, analysis of variance followed by the Holm-Sidak test, where appropriate.
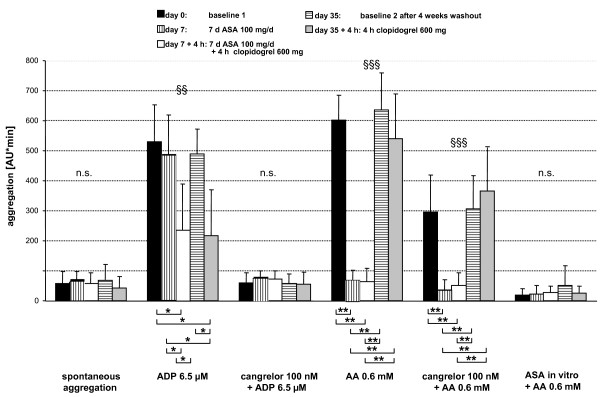
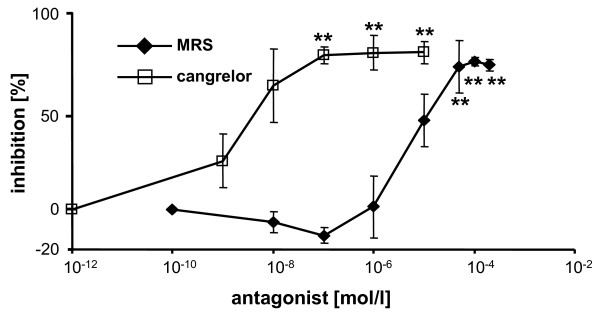
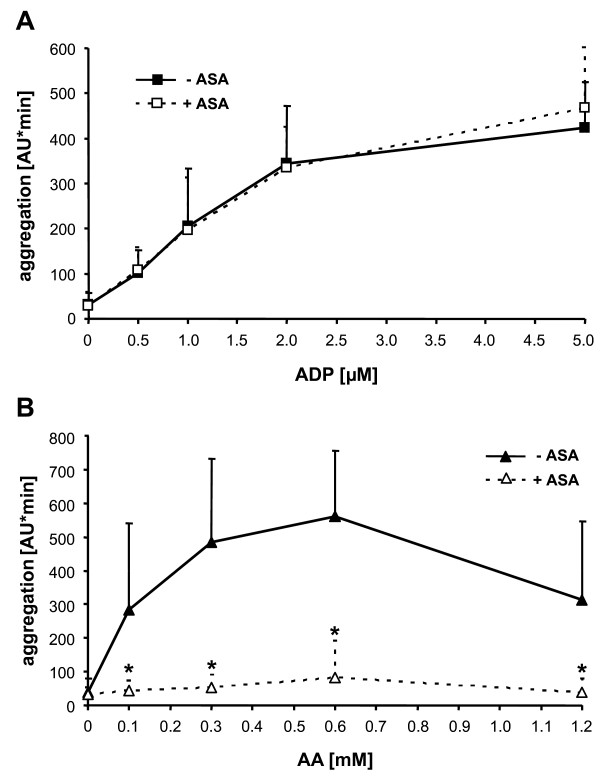
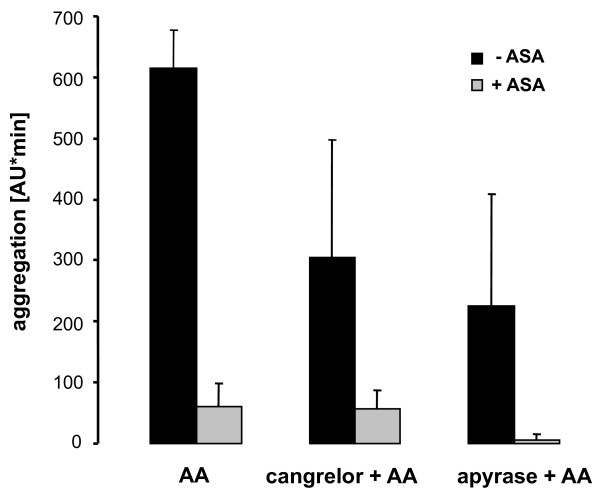
ADP-induced platelet aggregation in hirudin-anticoagulated blood was inhibited by 99.3 +/- 1.4% by in vitro addition of cangrelor (100 nM; p < 0.001) and by 64 +/- 35% by oral clopidogrel (600 mg) intake (p < 0.05; values are means +/- SD). Pre-incubation of blood with aspirin (1 mM) or oral aspirin intake (100 mg/day for 1 week) inhibited arachidonic acid (AA)-stimulated aggregation >95% and 100 +/- 3.2%, respectively (p < 0.01). Aspirin did not influence ADP-induced platelet aggregation, either in vitro or ex vivo. Oral intake of clopidogrel did not significantly reduce AA-induced aggregation, but P2Y12 blockade by cangrelor (100 nM) in vitro diminished AA-stimulated aggregation by 53 +/- 26% (p < 0.01). A feasibility study in healthy volunteers showed that dual anti-platelet drug intake (aspirin and clopidogrel) could be selectively monitored by MEA.
Selective platelet inhibition by aspirin and P2Y12 antagonists alone and in combination can be rapidly measured by MEA. We suggest that dual anti-platelet therapy with these two types of anti-platelet drugs can be optimized individually by measuring platelet responsiveness to ADP and AA with MEA before and after drug intake.
阿司匹林或氯吡格雷抑制血小板的效果不佳与心血管疾病患者的不良预后有关。目前缺乏可靠且简便的方法来测量阿司匹林和 P2Y12 拮抗剂治疗后的血小板抑制作用。多电极聚集仪(MEA)在临床研究中应用越来越广泛,它对阿司匹林和氯吡格雷抑制血小板敏感,但对 MEA 监测阿司匹林和 P2Y12 拮抗剂双联抗血小板治疗的效果评估不足。
通过进行体外和体内实验,我们评估了 MEA 监测 P2Y12 拮抗剂(体内氯吡格雷,体外坎格雷洛)和阿司匹林(体内每天 100mg,体外 1mM 或 5.4mM)单独及联合应用抑制血小板的可行性。统计分析采用曼-惠特尼秩和检验、学生 t 检验、方差分析和 Holm-Sidak 检验。
在肝素抗凝的血液中,ADP 诱导的血小板聚集被体外添加的坎格雷洛(100nM;p < 0.001)抑制 99.3 +/- 1.4%,被口服氯吡格雷(600mg)抑制 64 +/- 35%(p < 0.05;数值为平均值 +/- SD)。在体外孵育血液时,阿司匹林(1mM)或口服阿司匹林(每天 100mg 连续 1 周)抑制花生四烯酸(AA)刺激的聚集分别大于 95%和 100 +/- 3.2%(p < 0.01)。阿司匹林在体外或体内均不影响 ADP 诱导的血小板聚集。口服氯吡格雷不能显著减少 AA 诱导的聚集,但体外坎格雷洛(100nM)抑制 P2Y12 阻断可使 AA 刺激的聚集减少 53 +/- 26%(p < 0.01)。在健康志愿者的可行性研究中,我们发现 MEA 可选择性监测阿司匹林和氯吡格雷的双联抗血小板药物。
MEA 可快速测量阿司匹林和 P2Y12 拮抗剂单独和联合应用的选择性血小板抑制作用。我们建议,通过在药物摄入前后使用 MEA 测量对 ADP 和 AA 的血小板反应性,可优化这两种类型的抗血小板药物的双联抗血小板治疗。