Chowdhry Saeed, Hazani Ron, Collis Philip, Wilhelmi Bradon J
University of Louisville, Louisville, KY 40241.
Eplasty. 2010 May 28;10:e41.
Breast reconstruction techniques have focused increasingly on using autologous tissue, with emphasis being placed on employing muscle sparing adipocutaneous flaps to reduce abdominal wall complications such as hernias, bulges, weakness, and length of hospital stay. The result has been the emergence of the deep inferior epigastric perforator (DIEP) flap for breast reconstruction. Isolating perforator vessels challenges most surgeons. We describe surface anatomical landmarks to predict the location of the deep inferior epigastric artery (DIEA) and its perforators to aid in the efficient elevation of this flap.
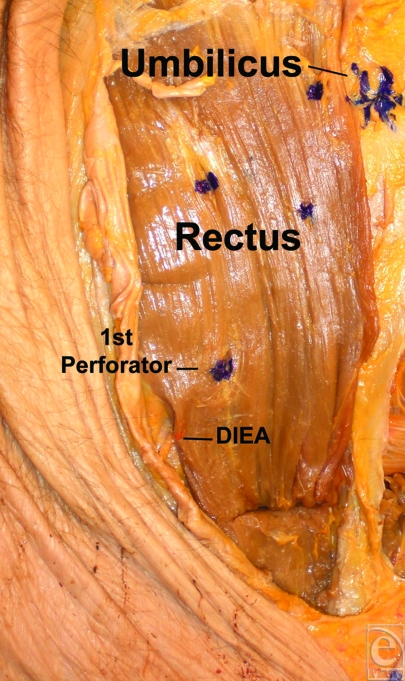
Ten fresh hemi-abdomens were dissected with loupe magnification. The DIEA and its perforators were identified, and measurements in relation to the rectus muscle, xiphoid, umbilicus, and pubis were taken. Statistical analysis was undertaken to determine distance ratios to account for variance in patient size.
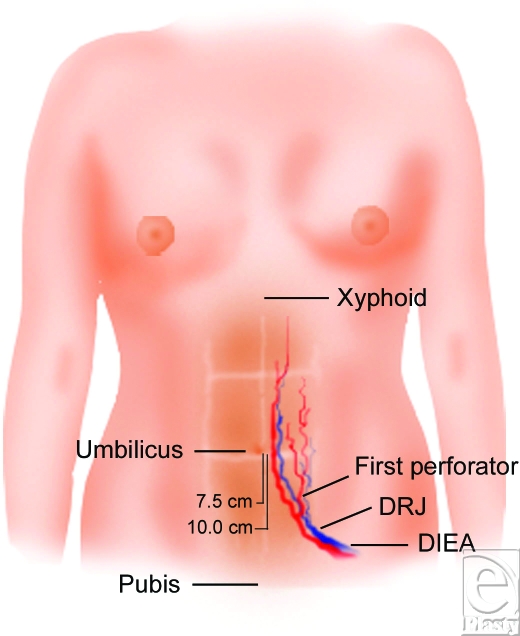
Average distance from the xiphoid to umbilicus was 18.2 +/- 1.27 cm. The distance from the umbilicus to pubis was 14.9 +/- 2.3 cm. The vertical distance from the umbilicus to the DRJ (DIEA rtctus junction) was 10.45 +/- 1.58 cm, and the vertical distance from the level of the umbilicus to where the first DIEA perforator traverses the RAM was 7.4 +/- 1.64 cm. The distance between the umbilicus and the DRJ is approximately 0.7 times the distance between the umbilicus and the pubic symphysis. The distance between the umbilicus and the first perforator is approximately 0.5 times the distance between the umbilicus and the pubic symphysis.
Knowledge of anatomical landmarks can aid the surgeon in more efficiently harvesting the DIEP flap. Surface landmarks along the abdominal midline coupled with normalizing ratios can aid surgeons in predicting the location of the DIEA and its first perforator. The DIEA crosses the rectus at approximately two thirds of the distance between the umbilicus and pubis, and the first perforator can reliably be located at one half of this distance.
乳房重建技术越来越多地专注于使用自体组织,重点是采用保留肌肉的脂肪皮瓣,以减少腹壁并发症,如疝气、隆起、薄弱和缩短住院时间。结果是出现了用于乳房重建的腹壁下深动脉穿支(DIEP)皮瓣。分离穿支血管对大多数外科医生来说是一项挑战。我们描述了表面解剖标志,以预测腹壁下深动脉(DIEA)及其穿支的位置,以帮助高效掀起该皮瓣。
用放大镜解剖10个新鲜半腹部。识别DIEA及其穿支,并测量与腹直肌、剑突、脐和耻骨的关系。进行统计分析以确定距离比,以考虑患者体型的差异。
剑突到脐的平均距离为18.2±1.27厘米。脐到耻骨的距离为14.9±2.3厘米。脐到DIEA-腹直肌交界处(DRJ)的垂直距离为10.45±1.58厘米,脐水平到第一个DIEA穿支穿过腹直肌后鞘(RAM)处的垂直距离为7.4±1.64厘米。脐与DRJ之间的距离约为脐与耻骨联合之间距离的0.7倍。脐与第一个穿支之间的距离约为脐与耻骨联合之间距离的0.5倍。
了解解剖标志可帮助外科医生更高效地切取DIEP皮瓣。腹部中线的表面标志以及标准化比例可帮助外科医生预测DIEA及其第一个穿支的位置。DIEA在脐与耻骨之间距离的约三分之二处穿过腹直肌,第一个穿支可可靠地定位在该距离的一半处。