Department of Cardiology and Angiology, University Hospital of Freiburg, Hugstetter Str 55, 79106 Freiburg im Breisgau, Germany.
Crit Care. 2010;14(3):R104. doi: 10.1186/cc9050. Epub 2010 Jun 4.
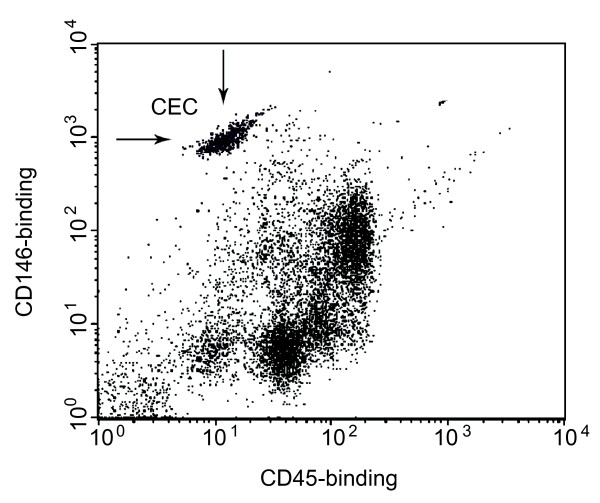
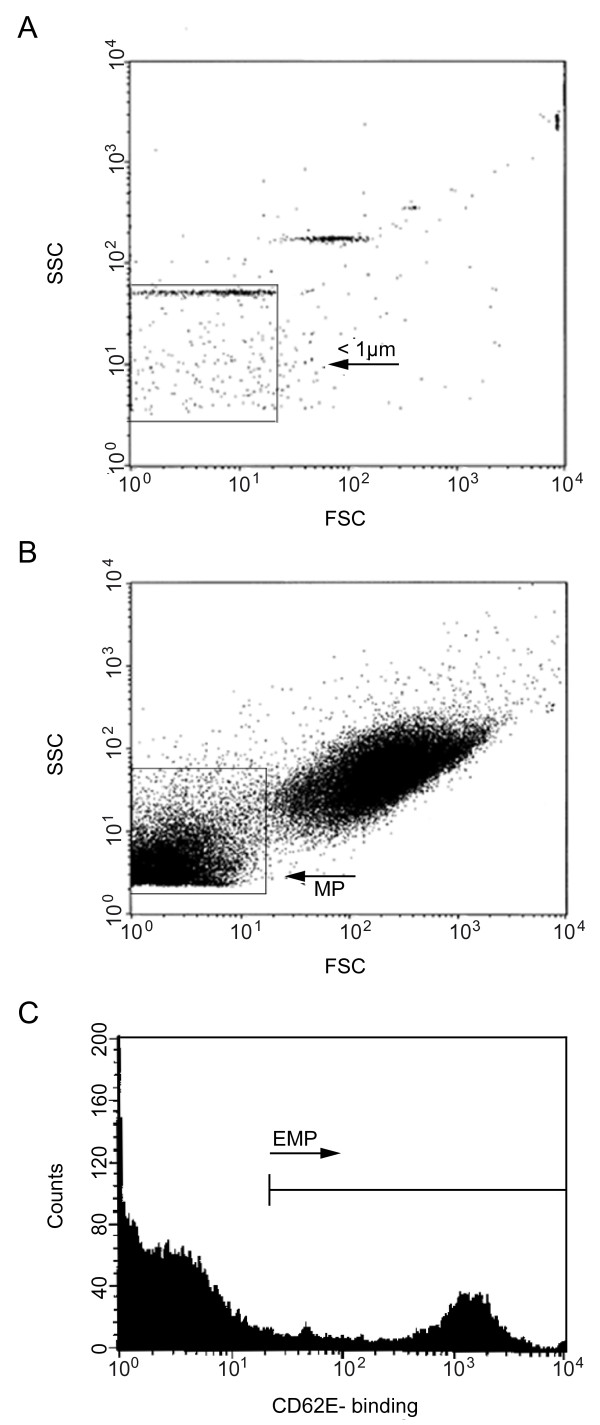
Ischemia and reperfusion after cardiopulmonary resuscitation (CPR) induce endothelial activation and systemic inflammatory response, resulting in post-resuscitation disease. In this study we analyzed direct markers of endothelial injury, circulating endothelial cells (CECs) and endothelial microparticles (EMPs), and endothelial progenitor cells (EPCs) as a marker of endothelial repair in patients after CPR.
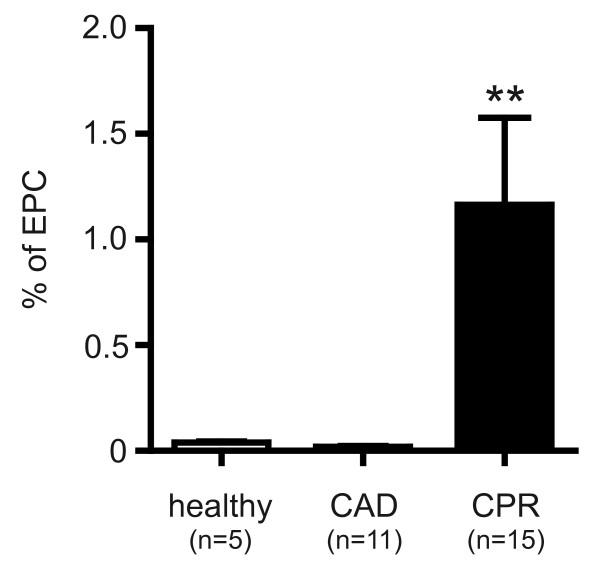
First we investigated endothelial injury in 40 patients after CPR, 30 controls with stable coronary artery disease (CAD), and 9 healthy subjects, who were included to measure CECs and EMPs. In a subsequent study, endothelial repair was assessed by EPC measurement in 15 CPR, 9 CAD, and 5 healthy subjects. Blood samples were drawn immediately and 24 hours after ROSC and analyzed by flow cytometry. For all statistical analyses P < 0.05 was considered significant.
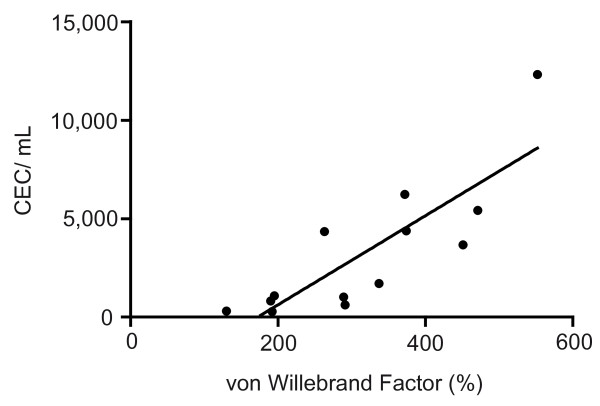
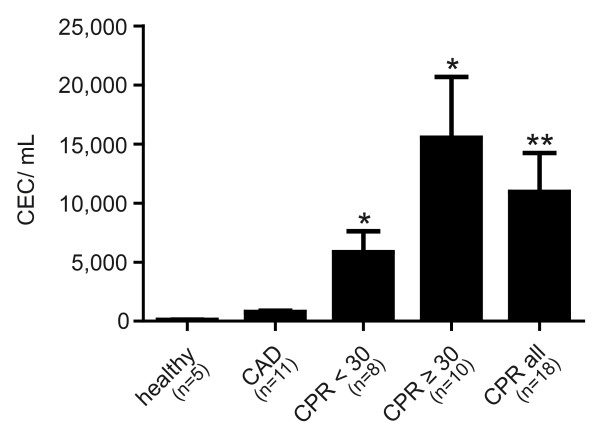
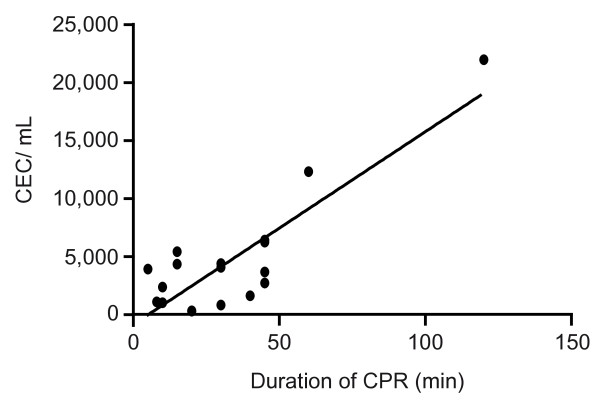
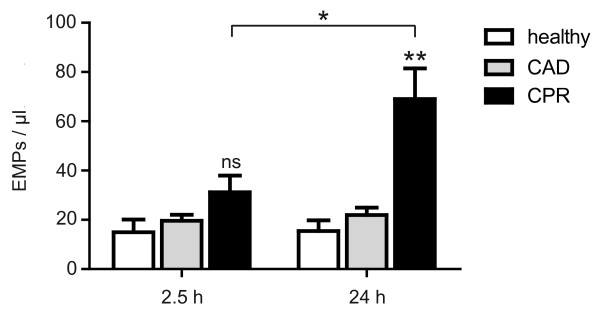
There was a massive rise in CEC count in resuscitated patients compared to CAD (4,494.1 +/- 1,246 versus 312.7 +/- 41 cells/mL; P < 0.001) and healthy patients (47.5 +/- 3.7 cells/mL; P < 0.0005). Patients after prolonged CPR (>or=30 min) showed elevated CECs compared to those resuscitated for <30 min (6,216.6 +/- 2,057 versus 2,340.9 +/- 703.5 cells/mL; P = 0.13/ns). There was a significant positive correlation of CEC count with duration of CPR (R2= 0.84; P < 0.01). EMPs were higher immediately after CPR compared to controls (31.2 +/- 5.8 versus 19.7 +/- 2.4 events/microL; P = 0.12 (CAD); versus 15.0 +/- 5.2 events/microL; P = 0.07 (healthy)) but did not reach significance until 24 hours after CPR (69.1 +/- 12.4 versus 22.0 +/- 3.0 events/microL; P < 0.005 (CAD); versus 15.4 +/- 4.4 events/microL; P < 0.001 (healthy)). EPCs were significantly elevated in patients on the second day after CPR compared to CAD (1.16 +/- 0.41 versus 0.02 +/- 0.01% of lymphocytes; P < 0.005) and healthy (0.04 +/- 0.01; P < 0.005).
In the present study we provide evidence for a severe endothelial damage after successful CPR. Our results point to an ongoing process of endothelial injury, paralleled by a subsequent endothelial regeneration 24 hours after resuscitation.
心肺复苏(CPR)后的缺血再灌注会引起内皮细胞激活和全身炎症反应,导致复苏后疾病。在这项研究中,我们分析了直接的内皮损伤标志物,循环内皮细胞(CEC)和内皮细胞微颗粒(EMP),以及内皮祖细胞(EPC)作为 CPR 后患者内皮修复的标志物。
首先,我们研究了 40 名 CPR 后患者、30 名稳定性冠状动脉疾病(CAD)对照患者和 9 名健康受试者的内皮损伤,这些患者被纳入以测量 CEC 和 EMP。在随后的研究中,通过测量 15 名 CPR、9 名 CAD 和 5 名健康受试者的 EPC 来评估内皮修复。在 ROSC 后立即和 24 小时采集血液样本,并通过流式细胞术进行分析。所有统计分析均认为 P < 0.05 具有统计学意义。
与 CAD(4494.1 +/- 1246 与 312.7 +/- 41 个/mL;P < 0.001)和健康患者(47.5 +/- 3.7 个/mL;P < 0.0005)相比,复苏患者的 CEC 计数大量增加。与 CPR < 30 分钟的患者相比,CPR > 30 分钟的患者的 CEC 升高(6216.6 +/- 2057 与 2340.9 +/- 703.5 个/mL;P = 0.13/无显著性差异)。CEC 计数与 CPR 时间呈显著正相关(R2= 0.84;P < 0.01)。与对照组相比,CPR 后 EMP 立即升高(31.2 +/- 5.8 与 19.7 +/- 2.4 个/微升;P = 0.12(CAD);与 15.0 +/- 5.2 个/微升;P = 0.07(健康)),但直到 CPR 后 24 小时才达到显著水平(69.1 +/- 12.4 与 22.0 +/- 3.0 个/微升;P < 0.005(CAD);与 15.4 +/- 4.4 个/微升;P < 0.001(健康))。CPR 后第二天,患者的 EPC 明显升高,与 CAD(1.16 +/- 0.41 与 0.02 +/- 0.01%的淋巴细胞;P < 0.005)和健康(0.04 +/- 0.01;P < 0.005)相比。
本研究为成功 CPR 后内皮严重损伤提供了证据。我们的结果表明内皮损伤持续存在,同时在复苏后 24 小时内皮再生。