Adams Jose A, Uryash Arkady, Lopez Jose R
Division of Neonatology, Mount Sinai Medical Center, Miami Beach, FL 33140, USA.
Department of Research, Mount Sinai Medical Center, Miami Beach, FL 33140, USA.
Biomedicines. 2022 Nov 28;10(12):3050. doi: 10.3390/biomedicines10123050.
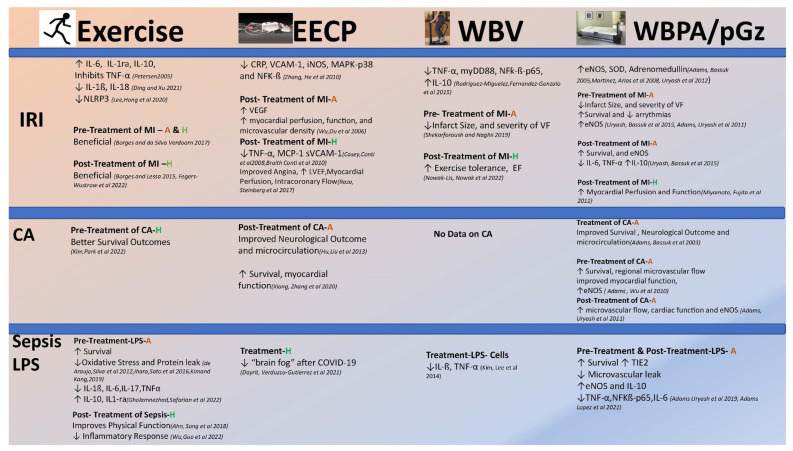
The monolayer of cells that line both the heart and the entire vasculature is the endothelial cell (EC). These cells respond to external and internal signals, producing a wide array of primary or secondary messengers involved in coagulation, vascular tone, inflammation, and cell-to-cell signaling. Endothelial cell activation is the process by which EC changes from a quiescent cell phenotype, which maintains cellular integrity, antithrombotic, and anti-inflammatory properties, to a phenotype that is prothrombotic, pro-inflammatory, and permeable, in addition to repair and leukocyte trafficking at the site of injury or infection. Pathological activation of EC leads to increased vascular permeability, thrombosis, and an uncontrolled inflammatory response that leads to endothelial dysfunction. This pathological activation can be observed during ischemia reperfusion injury (IRI) and sepsis. Shear stress (SS) and pulsatile shear stress (PSS) are produced by mechanical frictional forces of blood flow and contraction of the heart, respectively, and are well-known mechanical signals that affect EC function, morphology, and gene expression. PSS promotes EC homeostasis and cardiovascular health. The archetype of inducing PSS is exercise (i.e., jogging, which introduces pulsations to the body as a function of the foot striking the pavement), or mechanical devices which induce external pulsations to the body (Enhanced External Pulsation (EECP), Whole-body vibration (WBV), and Whole-body periodic acceleration (WBPA aka pGz)). The purpose of this narrative review is to focus on the aforementioned noninvasive methods to increase PSS, review how each of these modify specific diseases that have been shown to induce endothelial activation and microcirculatory dysfunction (Ischemia reperfusion injury-myocardial infarction and cardiac arrest and resuscitation), sepsis, and lipopolysaccharide-induced sepsis syndrome (LPS)), and review current evidence and insight into how each may modify endothelial activation and how these may be beneficial in the acute and chronic setting of endothelial activation and microvascular dysfunction.
构成心脏和整个脉管系统内壁的单层细胞是内皮细胞(EC)。这些细胞对外界和内部信号作出反应,产生一系列参与凝血、血管张力、炎症和细胞间信号传导的一级或二级信使。内皮细胞激活是指内皮细胞从维持细胞完整性、抗血栓形成和抗炎特性的静止细胞表型转变为促血栓形成、促炎和具有通透性的表型的过程,此外还涉及损伤或感染部位的修复和白细胞运输。内皮细胞的病理性激活会导致血管通透性增加、血栓形成以及导致内皮功能障碍的失控性炎症反应。这种病理性激活在缺血再灌注损伤(IRI)和脓毒症期间可以观察到。剪切应力(SS)和脉动剪切应力(PSS)分别由血流的机械摩擦力和心脏收缩产生,是影响内皮细胞功能、形态和基因表达的著名机械信号。PSS促进内皮细胞稳态和心血管健康。诱导PSS的典型方式是运动(即慢跑,随着脚与路面接触,身体会产生脉动),或向身体施加外部脉动的机械设备(增强型体外反搏(EECP)、全身振动(WBV)和全身周期性加速(WBPA,又名pGz))。本叙述性综述的目的是聚焦于上述增加PSS的非侵入性方法,回顾每种方法如何改善已被证明会诱导内皮激活和微循环功能障碍的特定疾病(缺血再灌注损伤——心肌梗死、心脏骤停与复苏)、脓毒症以及脂多糖诱导的脓毒症综合征(LPS),并回顾当前关于每种方法如何改善内皮激活以及在急性和慢性内皮激活及微血管功能障碍情况下这些方法可能如何有益的证据和见解。