i3 Innovus, Eden Prairie, Minnesota, USA.
BMC Psychiatry. 2010 Jun 4;10:39. doi: 10.1186/1471-244X-10-39.
Previous research has documented that the symptoms of bipolar disorder are often mistaken for unipolar depression prior to a patient's first bipolar diagnosis. The assumption has been that once a patient receives a bipolar diagnosis they will no longer be given a misdiagnosis of depression. The objectives of this study were 1) to assess the rate of subsequent unipolar depression diagnosis in individuals with a history of bipolar disorder and 2) to assess the increased cost associated with this potential misdiagnosis.
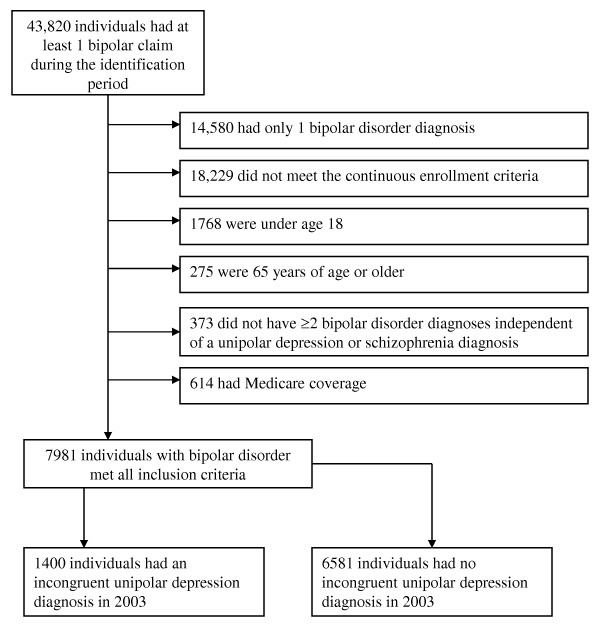
This study utilized a retrospective cohort design using administrative claims data from 2002 and 2003. Patient inclusion criteria for the study were 1) at least 2 bipolar diagnoses in 2002, 2) continuous enrollment during 2002 and 2003, 3) a pharmacy benefit, and 4) age 18 to 64. Patients with at least 2 unipolar depression diagnoses in 2003 were categorized as having an incongruent diagnosis of unipolar depression. We used propensity scoring to control for selection bias. Utilization was evaluated using negative binomial models. We evaluated cost differences between patient cohorts using generalized linear models.
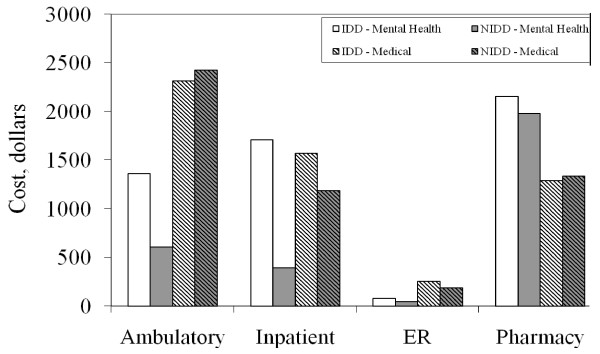
Of the 7981 patients who met all inclusion criteria for the analysis, 17.5% (1400) had an incongruent depression diagnosis (IDD). After controlling for background differences, individuals who received an IDD had higher rates of inpatient and outpatient psychiatric utilization and cost, on average, an additional $1641 per year compared to individuals without an IDD.
A strikingly high proportion of bipolar patients are given the differential diagnosis of unipolar depression after being identified as having bipolar disorder. Individuals with an IDD had increased acute psychiatric care services, suggesting higher levels of relapses, and were at risk for inappropriate treatment, as antidepressant therapy without a concomitant mood-stabilizing medication is contraindicated in bipolar disorder. Further prospective research is needed to validate the findings from this retrospective administrative claims-based analysis.
先前的研究表明,在患者首次被诊断为双相障碍之前,其症状常常被误诊为单相抑郁。人们曾认为,一旦患者被诊断为双相障碍,他们将不再被误诊为抑郁症。本研究的目的是:1)评估有双相障碍病史的个体随后被诊断为单相抑郁的比率;2)评估这种潜在误诊相关的费用增加。
本研究使用回顾性队列设计,利用 2002 年和 2003 年的行政索赔数据。研究纳入标准为:1)2002 年至少有 2 次双相诊断;2)2002 年和 2003 年连续入组;3)有药房福利;4)年龄 18-64 岁。2003 年至少有 2 次单相抑郁诊断的患者被归类为患有单相抑郁的不一致诊断。我们使用倾向评分来控制选择偏倚。利用负二项式模型评估利用情况。我们使用广义线性模型评估两组患者的成本差异。
在符合分析纳入标准的 7981 名患者中,17.5%(1400 人)患有不一致的抑郁诊断(IDD)。在控制背景差异后,与没有 IDD 的患者相比,患有 IDD 的患者的住院和门诊精神科就诊率和费用更高,平均每年增加 1641 美元。
在被诊断为双相障碍后,相当高比例的双相患者被给予单相抑郁的鉴别诊断。患有 IDD 的患者急性精神科服务利用率增加,提示复发率较高,且存在治疗不当的风险,因为在双相障碍中,抗抑郁药物治疗没有伴随心境稳定剂是禁忌的。需要进一步的前瞻性研究来验证基于回顾性行政索赔分析的研究结果。