Department of Social Medicine, School of Health Management, Harbin Medical University, 157 Baojian Road, Harbin City, Heilongjiang Province, China.
BMC Health Serv Res. 2010 Jun 17;10:170. doi: 10.1186/1472-6963-10-170.
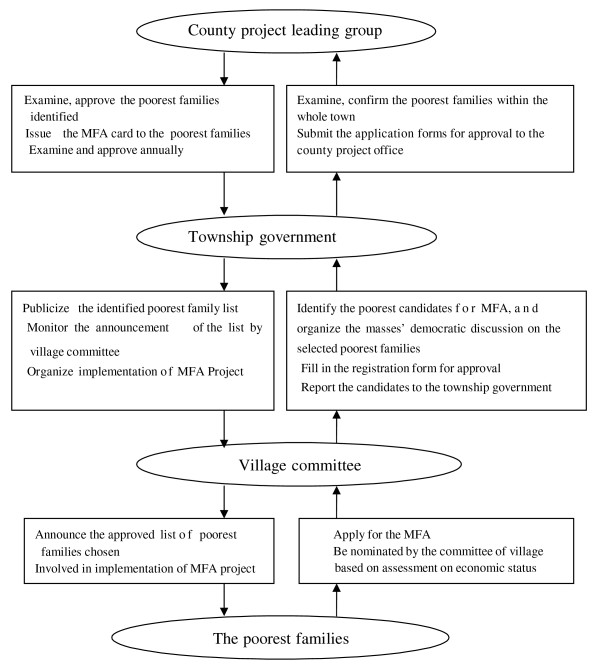
Since 2003 and 2005, National Pilot Medical Financial Assistance Scheme (MFA) has been implemented in rural and urban areas of China to improve the poorest families' accessibility to health services. Local governments of the pilot areas formulated various benefit packages. Comparative evaluation research on the effect of different benefit packages is urgently needed to provide evidence for improving policy-making of MFA. This study was based on a MFA pilot project, which was one component of Health VIII Project conducted in rural China. This article aimed to compare difference in health services utilization of poor families between two benefit package project areas: H8 towns (package covering inpatient service, some designated preventive and curative health services but without out-patient service reimbursement in Health VIII Project,) and H8SP towns (package extending coverage of target population, covering out- patient services and reducing co-payment rate in Health VIII Supportive Project), and to find out major influencing factors on their services utilization.
A cross-sectional survey was conducted in 2004, which used stratified cluster sampling method to select poor families who have been enrolled in MFA scheme in rural areas of ChongQing. All family members of the enrolled households were interviewed. 748 and 1129 respondents from two kinds of project towns participated in the survey. Among them, 625 and 869 respondents were included (age>/=15) in the analysis of this study. Two-level linear multilevel model and binomial regressions with a log link were used to assess influencing factors on different response variables measuring service utilization.
In general, there was no statistical significance in physician visits and hospitalizations among all the respondents between the two kinds of benefit package towns. After adjusting for major confounding factors, poor families in H8SP towns had much higher frequency of MFA use (beta = 1.17) and less use of hospitalization service (OR = 0.7 (H8SP/H8), 95%CI (0.5, 1.0)) among all the respondents. While calculating use of hospital services among those who needed, there was significant difference (p = 0.032) in percentage of hospitalization use between H8SP towns (46%) and H8 towns (33%). Meanwhile, the non-use but ought-to-use hospitalization ratio of H8SP (54%) was lower than that of H8 (67 %) towns. This indicated that hospitalization utilizations had improved in H8SP towns among those who needed. Awareness of MFA detailed benefit package and presence of physician diagnosed chronic disease had significant association with frequency of MFA use and hospitalizations. There was no significant difference in rate of borrowing money for illness treatment between the two project areas. Large amount of medical debt had strong association with hospitalization utilization.
The new extended benefit package implemented in pilot towns significantly increased the poor families' accessibility to MFA package in H8SP than that of H8 towns, which reduced poor families' demand of hospitalization services for their chronic diseases, and improved the poor population's utilization of out-patient services to some degree. It can encourage poor people to use more outpatient services thus reduce their hospitalization need. Presence of chronic disease and hospitalization had strong association with the presence of large amount of medical debt, which indicated that: although establishment of MFA had facilitated accessibility of poor families to this new system, and improved service utilization of poor families to some degree, but its role in reducing poor families' medical debt resulted from chronic disease and hospitalization was still very limited. Besides, the following requirements of MFA: co-payment for in-patient services, ceiling and deductibles for reimbursement, limitations on eligibility for diseases reimbursement, also served as most important obstacles for poor families' access to health care. Therefore, there is great need to improve MFA benefit package design in the future, including extending to cover out-patient services, raising ceiling for reimbursement, removing deductibles of MFA, reducing co-payment rate, and integrating MFA with New Rural Cooperative Medical Scheme more closely so as to provide more protection to the poor families.
自 2003 年和 2005 年以来,中国在农村和城市地区实施了国家试点医疗财政援助计划(MFA),以改善最贫困家庭获得卫生服务的机会。试点地区的地方政府制定了各种福利套餐。迫切需要对不同福利套餐的效果进行比较评估研究,为 MFA 政策制定提供证据。本研究基于 MFA 试点项目,该项目是中国农村卫生八项目的一个组成部分。本文旨在比较贫困家庭在两个福利套餐项目地区之间的卫生服务利用情况的差异:H8 镇(套餐涵盖住院服务、一些指定的预防和治疗性卫生服务,但在卫生八项目中不包括门诊服务报销)和 H8SP 镇(套餐扩大目标人群的覆盖范围,涵盖门诊服务,并降低卫生八支持项目的共付率),并找出影响其服务利用的主要因素。
2004 年进行了一项横断面调查,采用分层聚类抽样方法选择在重庆市农村地区参加 MFA 计划的贫困家庭。对所有被登记家庭的成员进行了访谈。来自两种项目镇的 748 名和 1129 名受访者参加了调查。其中,625 名和 869 名受访者(年龄>/=15 岁)被纳入本研究的分析。使用两级线性多水平模型和双变量回归与对数链接来评估不同反应变量(衡量服务利用情况)的影响因素。
总体而言,在所有受访者中,两种福利套餐镇之间的就诊和住院次数没有统计学意义。在调整了主要混杂因素后,H8SP 镇的贫困家庭 MFA 使用频率更高(beta = 1.17),住院服务使用率更低(OR = 0.7(H8SP/H8),95%CI(0.5,1.0))。在计算需要住院服务的人中,H8SP 镇(46%)和 H8 镇(33%)的住院服务使用率存在显著差异(p = 0.032)。同时,H8SP 镇(54%)的非使用但应使用住院服务的比例低于 H8 镇(67%)。这表明,在 H8SP 镇,需要住院服务的人中,住院服务的利用情况有所改善。对 MFA 详细福利套餐的认识和医生诊断的慢性疾病的存在与 MFA 使用频率和住院治疗有显著关联。两个项目地区的因病借款率没有显著差异。大量的医疗债务与住院利用有很强的关联。
在试点镇实施的新扩展福利套餐显著增加了 H8SP 镇贫困家庭获得 MFA 套餐的机会,这降低了贫困家庭对慢性疾病住院服务的需求,并在一定程度上改善了贫困人口对门诊服务的利用。它可以鼓励穷人更多地使用门诊服务,从而减少他们对住院的需求。慢性疾病和住院治疗与大量医疗债务之间存在很强的关联,这表明:尽管 MFA 的建立促进了贫困家庭对这一新系统的获得,在一定程度上改善了贫困家庭的服务利用,但它在减轻贫困家庭因慢性疾病和住院治疗而产生的医疗债务方面的作用仍然非常有限。此外,MFA 的以下要求:住院服务的共付额、报销的上限和免赔额、疾病报销资格的限制,也是贫困家庭获得医疗保健的最重要障碍。因此,今后有必要改进 MFA 福利套餐设计,包括扩大门诊服务范围、提高报销上限、取消 MFA 的免赔额、降低共付率,并使 MFA 与新型农村合作医疗制度更加紧密地结合,以更好地为贫困家庭提供保障。