Department of Trauma-, Hand- and Reconstructive Surgery Friedrich Schiller University Jena, Germany.
BMC Musculoskelet Disord. 2010 Jul 7;11:153. doi: 10.1186/1471-2474-11-153.
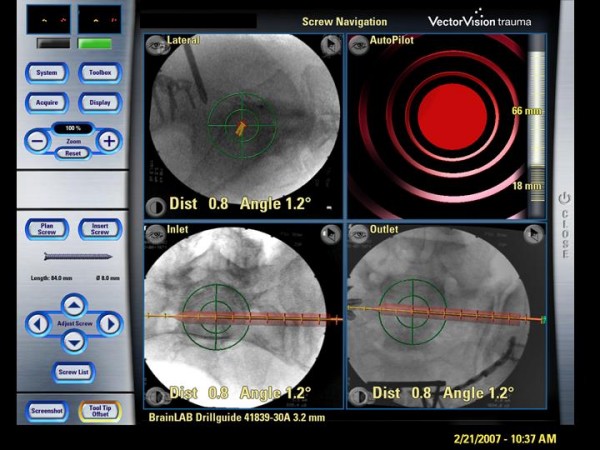
Screw fixation of pelvic ring fractures is a common, but demanding procedure and navigation techniques were introduced to increase the precision of screw placement. The purpose of this case series was the evaluation of screw misplacement rate and functional outcome of percutaneous screw fixation of pelvic ring disruptions using a 2D navigation system.
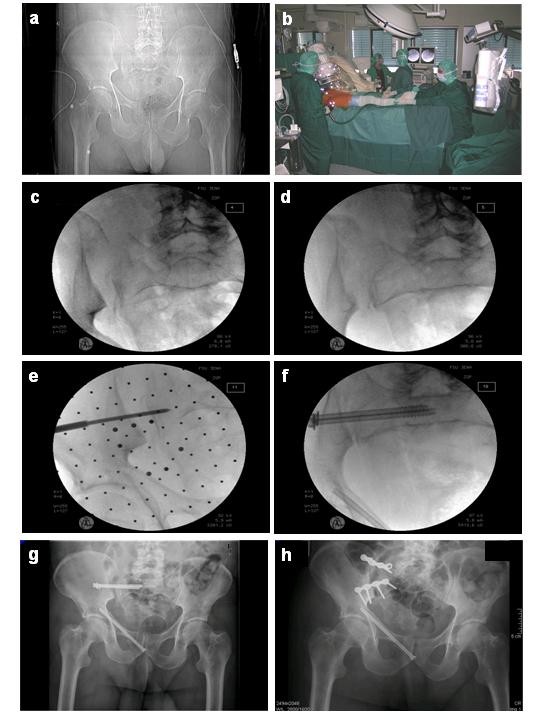
Between August 2004 and December 2007, 44 of 442 patients with pelvic injuries were included for closed reduction and percutaneous screw fixation of disrupted pelvic ring lesions using an optoelectronic 2D-fluoroscopic based navigation system. Operating and fluoroscopy time were measured, as well as peri- and postoperative complications documented. Screw position was assessed by postoperative CT scans. Quality of live was evaluated by SF 36-questionnaire in 40 of 44 patients at mean follow up 15.5 +/- 1.2 month.
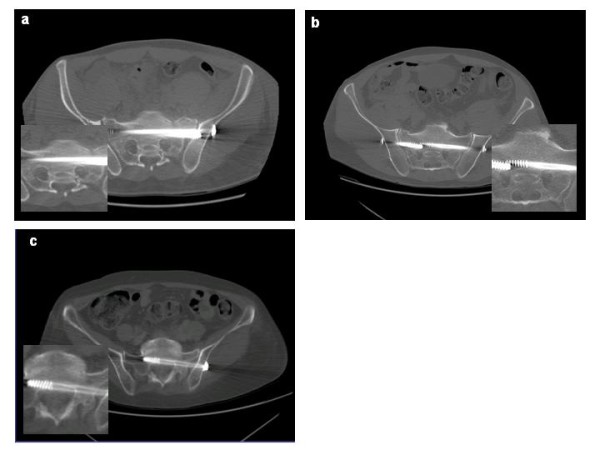
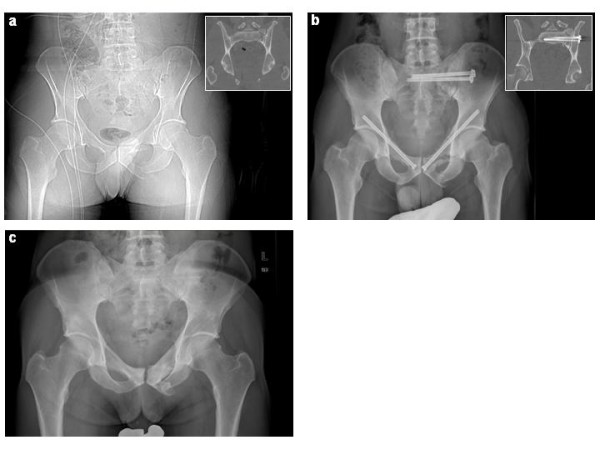
56 iliosacral- and 29 ramus pubic-screws were inserted (mean operation time per screw 62 +/- 4 minutes, mean fluoroscopy time per screw 123 +/- 12 seconds). In post-operative CT-scans the screw position was assessed and graded as follows: I. secure positioning, completely in the cancellous bone (80%); II. secure positioning, but contacting cortical bone structures (14%); III. malplaced positioning, penetrating the cortical bone (6%). The malplacements predominantly occurred in bilateral overlapping screw fixation. No wound infection or iatrogenic neurovascular damage were observed. Four re-operations were performed, two of them due to implant-misplacement and two of them due to implant-failure.
2D-fluoroscopic navigation is a safe tool providing high accuracy of percutaneous screw placement for pelvic ring fractures, but in cases of a bilateral iliosacral screw fixation an increased risk for screw misplacement was observed. If additional ramus pubic screw fixations are performed, the retrograde inserted screws have to pass the iliopubic eminence to prevent an axial screw loosening.
骨盆环骨折的螺钉固定是一种常见但要求较高的手术,导航技术的引入旨在提高螺钉放置的精度。本病例系列研究的目的是评估使用二维(2D)导航系统经皮固定骨盆环破裂时螺钉错位率和功能结果。
2004 年 8 月至 2007 年 12 月,44 例骨盆损伤患者接受了闭合复位和经皮固定骨盆环破裂的手术,使用光电二维(2D)荧光透视导航系统。测量手术和透视时间,并记录围手术期并发症。术后 CT 扫描评估螺钉位置。44 例患者中的 40 例在平均随访 15.5±1.2 个月时通过 SF-36 问卷评估生活质量。
共置入 56 枚骶髂螺钉和 29 枚耻骨支螺钉(每枚螺钉的平均手术时间为 62±4 分钟,每枚螺钉的平均透视时间为 123±12 秒)。术后 CT 扫描评估螺钉位置,分级如下:I. 安全定位,完全位于松质骨(80%);II. 安全定位,但接触皮质骨结构(14%);III. 定位不当,穿透皮质骨(6%)。这些定位不当主要发生在双侧重叠螺钉固定的情况下。未观察到伤口感染或医源性神经血管损伤。有 4 例患者进行了再手术,其中 2 例因植入物移位,2 例因植入物失败。
2D 荧光透视导航是一种安全的工具,为骨盆环骨折提供了经皮螺钉固定的高精度,但在双侧骶髂螺钉固定的情况下,螺钉错位的风险增加。如果进行额外的耻骨支螺钉固定,逆行插入的螺钉必须穿过髂耻隆起以防止轴向螺钉松动。