Department of Veterans Affairs New Jersey Healthcare System, East Orange, New Jersey, USA.
Diabetes Care. 2010 Oct;33(10):2133-9. doi: 10.2337/dc09-1665. Epub 2010 Jul 9.
To evaluate facility rankings in achieving <7% A1C levels based on the complexity of glycemic treatment regimens using threshold and continuous measures.
We conducted a retrospective administrative data analysis of Veterans Health Administration Medical Centers in 2003-2004. Eligible patients were identified using National Committee for Quality Assurance (NCQA) measure specifications. A complex glycemic regimen (CGR) was defined as receipt of insulin or three oral agents. Facilities were ranked using five ordinal categories based up both z score distribution and statistical significance (P < 0.05). Rankings using the NCQA definition were compared with a subset receiving CGRs using both a <7% threshold and a continuous measure awarding proportional credit for values between 7.9 and <7.0%. Ranking correlation was assessed using the Spearman correlation coefficient.
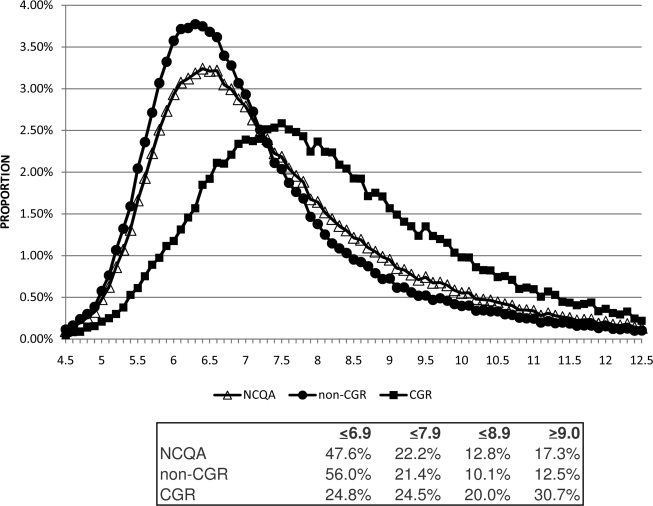
A total of 203,302 patients (mean age 55.2 years) were identified from 127 facilities (range 480-5,411, mean 1,601); 26.7% (17.9-35.2%) were receiving CGRs, including 22.0% receiving insulin. Mean A1C and percent achieving A1C <7% were 7.48 and 48% overall and 8.32 and 24.8% for those receiving CGRs using the threshold measure; proportion achieved was 60.1 and 37.2%, respectively, using the continuous measure. Rank correlation between the overall and CGR subset was 0.61; 8 of 24 of the highest or lowest ranked facilities changed to nonsignificance status; an additional five sites changed rankings.
Facility rankings in achieving the NCQA <7% measure as specified differ markedly from rankings using the CGR subset. Measurement for public reporting or payment should stratify rankings by CGR. A continuous measure may better align incentives with treatment intensity.
使用阈值和连续测量方法,根据血糖治疗方案的复杂性评估设施在达到 <7% A1C 水平方面的排名。
我们对 2003-2004 年退伍军人健康管理局医疗中心进行了回顾性行政数据分析。使用国家质量保证委员会 (NCQA) 测量规范确定合格患者。复杂血糖方案 (CGR) 的定义是接受胰岛素或三种口服药物。根据 z 分数分布和统计学意义 (P < 0.05),使用五个有序类别对设施进行排名。使用 NCQA 定义的排名与使用 <7% 阈值和连续测量方法为 7.9 至 <7.0% 之间的值授予比例信用的 CGR 子集进行比较。使用 Spearman 相关系数评估排名相关性。
从 127 家医疗机构(范围 480-5411,平均 1601)中确定了 203302 名患者(平均年龄 55.2 岁);26.7%(17.9-35.2%)接受 CGR,包括 22.0%接受胰岛素。总体而言,A1C 的平均值和达到 A1C <7%的百分比分别为 7.48%和 48%,对于使用阈值测量的接受 CGR 的患者分别为 8.32%和 24.8%;使用连续测量,分别为 60.1%和 37.2%。整体和 CGR 子集之间的排名相关性为 0.61;24 家排名最高或最低的医疗机构中有 8 家变为无统计学意义;另外五家机构的排名发生了变化。
根据 NCQA 规定的 <7% 测量值,医疗机构的排名与使用 CGR 子集的排名有很大差异。为了进行公共报告或支付,测量方法应按 CGR 对排名进行分层。连续测量可能会使激励措施与治疗强度更好地保持一致。