Singh Rupinder, Sen Indu, Wig Jyotsna, Minz M, Sharma Ashish, Bala Indu
Senior Resident, Department of Anaesthesia & Intensive care, and Department of Transplant Surgery, Post Graduate Institute of Medical Education & Research, Chandigarh, India, 160012.
Indian J Anaesth. 2009 Aug;53(4):434-41.
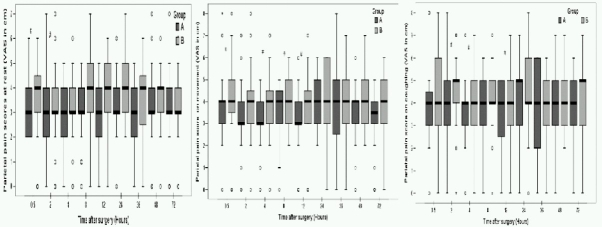
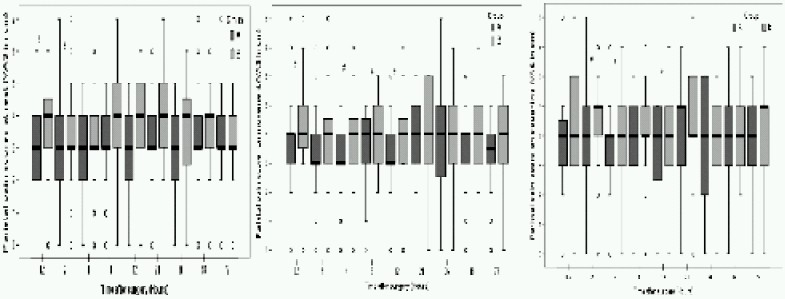
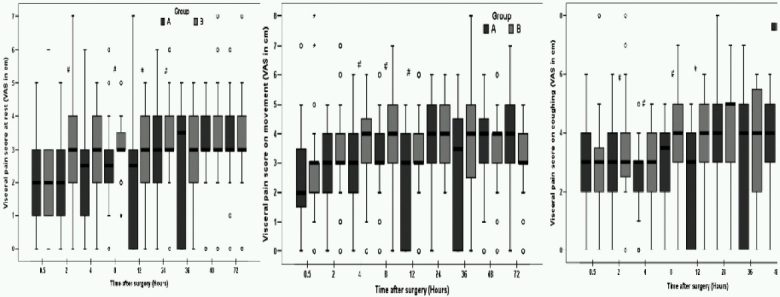
Choice of an appropriate anaesthetic technique and adequate pain relief during laparoscopic living donor nephrectomy (LDN) is likely to make the procedure more appealing to kidney donors. Various analgesic regimens proposed to relieve pain after laparoscopic surgery include: opioids, non-opioid analgesics followed by opioids for the breakthrough pain and intra-peritoneal normal saline irrigation and instillation of local anaesthetics at surgical sites. Thorough literature review and medline search did not reveal any study where a combination of orogastric acetazolamide along with intraperitoneal saline irrigation and bupivacaine instillation techniques have been tried in these patients. In a prospective, double blind, randomized trial, eighty healthy adults undergoing LDN under general anaesthesia were enrolled to compare the efficacy of an acetazolamide based multimodal analgesic approach (Group A) with conventional pain management (Group B). Donors' demographics, intra-operative variables, early allograft function and recovery characteristics were evaluated for 72 hours. The primary end points were postoperative pain intensity on a visual analog scale and the incidence of shoulder tip pain (STP). The secondary end points included the latency of the rescue analgesia request rate, total analgesic consumption and patient satisfaction. Consistently lower mean pain scores were observed in Group A (p<0.03 for visceral pain). Frequency as well as the total dose of rescue analgesics administered was significantly less in Group A (p=0.001). Twelve patients (30.7%) in Group B complained of STP compared to three (7.5%) in Group A (p=0.025). Shoulder pain also presented earlier (8 hours versus 12 hours) and persisted for longer period in Group B (72 hours versus 48 hours, p 0.025). To conclude, a multimodal analgesic approach consisting a combination of orogastric acetazolamide, intraperito-neal saline irrigation and use of bupivacaine in the operated renal fossa, pfannenstiel incision and laparoscopic port sites provide significant reduction in postoperative pain after LDN.
在腹腔镜活体供肾肾切除术(LDN)中选择合适的麻醉技术并实现充分的疼痛缓解,可能会使该手术对肾脏供体更具吸引力。为缓解腹腔镜手术后疼痛而提出的各种镇痛方案包括:阿片类药物、非阿片类镇痛药随后加用阿片类药物以缓解爆发性疼痛、腹腔内生理盐水冲洗以及在手术部位注入局部麻醉药。全面的文献综述和医学数据库检索未发现有研究在这些患者中尝试过胃内注射乙酰唑胺联合腹腔内生理盐水冲洗和布比卡因注入技术。在一项前瞻性、双盲、随机试验中,纳入了80例在全身麻醉下接受LDN的健康成年人,以比较基于乙酰唑胺的多模式镇痛方法(A组)与传统疼痛管理方法(B组)的疗效。对供体的人口统计学、术中变量、早期移植肾功能和恢复特征进行了72小时的评估。主要终点是视觉模拟量表上的术后疼痛强度和肩峰下疼痛(STP)的发生率。次要终点包括补救性镇痛请求率的潜伏期、总镇痛药物消耗量和患者满意度。A组的平均疼痛评分持续较低(内脏痛p<0.03)。A组使用的补救性镇痛药的频率和总剂量明显较少(p = 0.001)。B组有12例患者(30.7%)抱怨有STP,而A组为3例(7.5%)(p = 0.025)。B组的肩部疼痛出现也更早(8小时对12小时)且持续时间更长(72小时对48小时,p 0.025)。总之,一种由胃内注射乙酰唑胺、腹腔内生理盐水冲洗以及在手术的肾窝、耻骨上切口和腹腔镜穿刺部位使用布比卡因组成的多模式镇痛方法,可显著减轻LDN术后的疼痛。