University Department of Surgery, Faculty of Medicine, University of Glasgow, Glasgow, UK, G12 8RZ.
BMC Cancer. 2010 Jul 30;10:398. doi: 10.1186/1471-2407-10-398.
The long term outcome (more than 15 years) of adjuvant treatment in patients with primary operable breast cancer has rarely been examined.
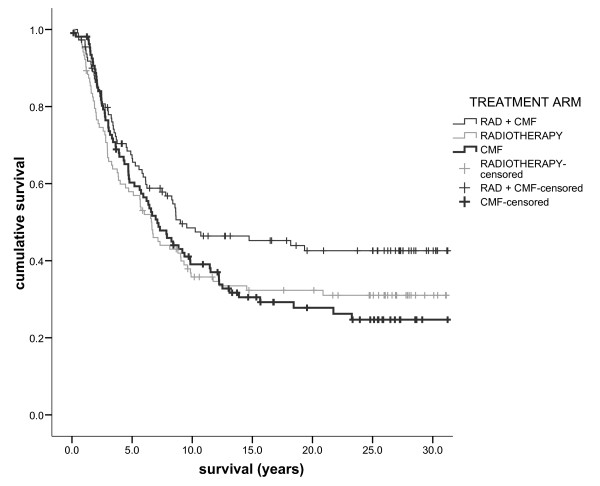
A randomised clinical trial of radiotherapy, chemotherapy (28 day cycles of cyclophosphamide, methotrexate and 5-fluorouracil) or both on women with primary operable breast cancer (n = 322) was followed-up for a median of 27 years.
260 (81%) patients died, 204 (78%) from breast cancer. Cancer specific survival (SE) at 10 years, 20 years and 30 years was 41 (3)%, 34 (3)% and 33 (3)% respectively. Presence of more than 3 involved lymph nodes increased cancer-specific mortality (HR 1.88, 95% CI 1.34-2.63) after adjustment for age, socio-economic deprivation and adjuvant treatment. Both age (HR 1.63, 95% CI 1.19-2.22) and involved lymph nodes (HR 1.59, 95% CI 1.17-2.14) were significant predictors of all-cause mortality after adjustment for other factors. There was no significant difference in all-cause or cancer-specific survival between patients in each of the 3 treatment arms.
The present study highlights the long term impact of node positive disease but does not indicate that any regimen was associated with significantly better long-term survival.
原发性可手术乳腺癌辅助治疗的长期结局(超过 15 年)很少被研究。
对原发性可手术乳腺癌患者(n = 322)进行了随机临床试验,比较了放疗、化疗(28 天周期的环磷酰胺、甲氨蝶呤和 5-氟尿嘧啶)或两者联合应用,中位随访时间为 27 年。
260 例(81%)患者死亡,204 例(78%)死于乳腺癌。10 年、20 年和 30 年的癌症特异性生存率(SE)分别为 41(3)%、34(3)%和 33(3)%。淋巴结受累超过 3 个的患者,在调整年龄、社会经济剥夺和辅助治疗后,癌症特异性死亡率增加(HR 1.88,95%CI 1.34-2.63)。在调整其他因素后,年龄(HR 1.63,95%CI 1.19-2.22)和淋巴结受累(HR 1.59,95%CI 1.17-2.14)是全因死亡率的显著预测因素。在每个治疗组中,全因或癌症特异性生存率均无显著差异。
本研究强调了阳性淋巴结疾病的长期影响,但并未表明任何方案与显著改善长期生存相关。