Department of Epidemiology and Biostatistics, University of California, San Francisco, San Francisco, California 94107, USA.
Ann Intern Med. 2010 Aug 3;153(3):137-46. doi: 10.7326/0003-4819-153-3-201008030-00004.
Dyslipidemia causes coronary heart disease in middle-aged and elderly adults, but the consequences of lipid exposure during young adulthood are unclear.
To assess whether nonoptimal lipid levels during young adulthood cause atherosclerotic changes that persist into middle age.
Prospective cohort study.
4 cities in the United States.
3258 participants from the 5115 black and white men and women recruited at age 18 to 30 years in 1985 to 1986 for the CARDIA (Coronary Artery Risk Development in Young Adults) study.
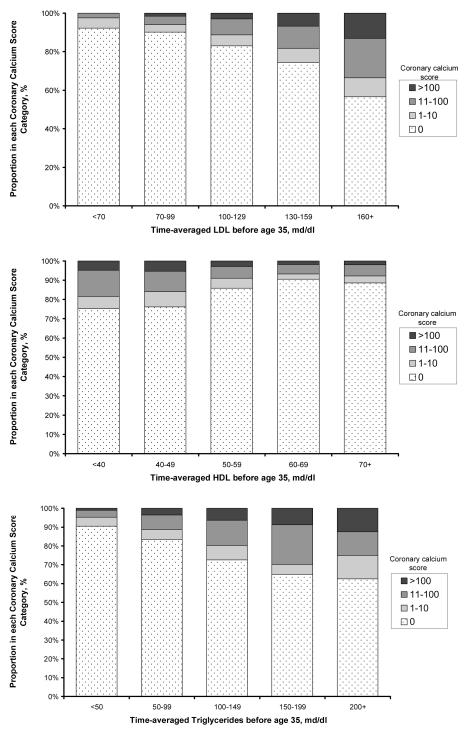
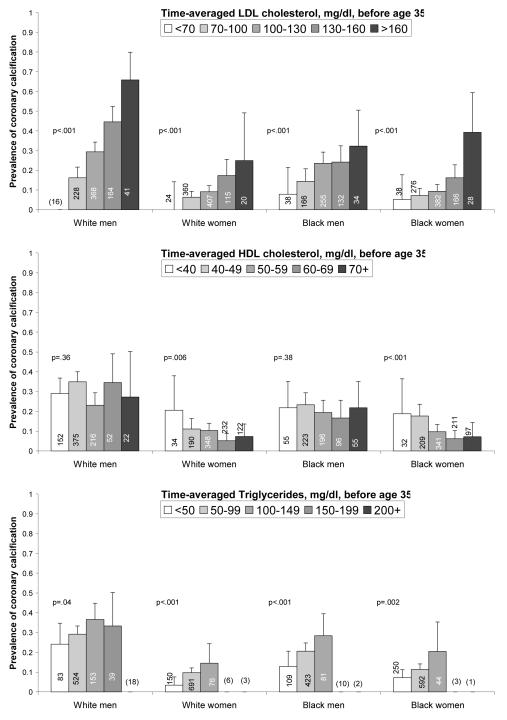
Low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol, triglycerides, and coronary calcium. Time-averaged cumulative exposures to lipids between age 20 and 35 years were estimated by using repeated serum lipid measurements over 20 years in the CARDIA study; these measurements were then related to coronary calcium scores assessed later in life (45 years [SD, 4]).
2824 participants (87%) had nonoptimal levels of LDL cholesterol (>or=2.59 mmol/L [>or=100 mg/dL]), HDL cholesterol (<1.55 mmol/L [<60 mg/dL]), or triglycerides (>or=1.70 mmol/L [>or=150 mg/dL]) during young adulthood. Coronary calcium prevalence 2 decades later was 8% in participants who maintained optimal LDL levels (<1.81 mmol/L [<70 mg/dL]), and 44% in participants with LDL cholesterol levels of 4.14 mmol/L (160 mg/dL) or greater (P < 0.001). The association was similar across race and sex and strongly graded, with odds ratios for coronary calcium of 1.5 (95% CI, 0.7 to 3.3) for LDL cholesterol levels of 1.81 to 2.56 mmol/L (70 to 99 mg/dL), 2.4 (CI, 1.1 to 5.3) for levels of 2.59 to 3.34 mmol/L (100 to 129 mg/dL), 3.3 (CI, 1.3 to 7.8) for levels of 3.37 to 4.12 mmol/L (130 to 159 mg/dL), and 5.6 (CI, 2.0 to 16) for levels of 4.14 mmol/L (160 mg/dL) or greater, compared with levels less than 1.81 mmol/L (<70 mg/dL), after adjustment for lipid exposure after age 35 years and other coronary risk factors. Both LDL and HDL cholesterol levels were independently associated with coronary calcium after participants who were receiving lipid-lowering medications or had clinically abnormal lipid levels were excluded.
Coronary calcium, although a strong predictor of future coronary heart disease, is not a clinical outcome.
Nonoptimal levels of LDL and HDL cholesterol during young adulthood are independently associated with coronary atherosclerosis 2 decades later.
National Heart, Lung, and Blood Institute.
血脂异常导致中老年人冠心病,但青年时期的血脂暴露后果尚不清楚。
评估青年时期非理想的血脂水平是否会导致持续到中年的动脉粥样硬化变化。
前瞻性队列研究。
美国 4 个城市。
1985 年至 1986 年,在 5115 名黑人和白人男性和女性中招募了年龄在 18 至 30 岁的 3258 名参与者参加 CARDIA(年轻人冠状动脉风险发展)研究。
低密度脂蛋白(LDL)和高密度脂蛋白(HDL)胆固醇、甘油三酯和冠状动脉钙。通过 CARDIA 研究中 20 年的重复血清脂质测量,估算出 20 岁至 35 岁之间的时间平均累积脂质暴露量;然后将这些测量值与以后的生活中评估的冠状动脉钙评分(45 岁[标准差,4])相关联。
2824 名参与者(87%)在青年时期有非理想的 LDL 胆固醇(>或=2.59 mmol/L[>或=100 mg/dL])、HDL 胆固醇(<1.55 mmol/L [<60 mg/dL])或甘油三酯(>或=1.70 mmol/L [>或=150 mg/dL])水平。20 年后,在 LDL 水平保持理想(<1.81 mmol/L [<70 mg/dL])的参与者中,冠状动脉钙的患病率为 8%,而 LDL 胆固醇水平为 4.14 mmol/L(160 mg/dL)或更高的参与者中,冠状动脉钙的患病率为 44%(P < 0.001)。这种关联在种族和性别之间相似,且呈明显梯度,LDL 胆固醇水平为 1.81 至 2.56 mmol/L(70 至 99 mg/dL)、2.59 至 3.34 mmol/L(100 至 129 mg/dL)、3.37 至 4.12 mmol/L(130 至 159 mg/dL)和 4.14 mmol/L(160 mg/dL)或更高的参与者与 LDL 胆固醇水平<1.81 mmol/L(<70 mg/dL)的参与者相比,患冠状动脉钙的比值比(OR)分别为 1.5(95%置信区间[CI],0.7 至 3.3)、2.4(CI,1.1 至 5.3)、3.3(CI,1.3 至 7.8)和 5.6(CI,2.0 至 16),这与年龄>35 岁后以及其他冠心病危险因素的脂质暴露情况调整后相比。在排除服用降脂药物或血脂水平异常的参与者后,LDL 和 HDL 胆固醇水平均与冠状动脉钙独立相关。
虽然冠状动脉钙是未来冠心病的一个强有力预测指标,但它并不是一种临床结果。
青年时期非理想的 LDL 和 HDL 胆固醇水平与 20 年后的冠状动脉粥样硬化独立相关。
美国国立心肺血液研究所。