Modi Hitesh N, Suh Seung-Woo, Hong Jae-Young, Song Sang-Heon, Yang Jae-Hyuk
Scoliosis Research Institute, Department of Orthopedics, Korea University Guro Hospital, Seoul, Korea.
Scoliosis. 2010 Aug 7;5:16. doi: 10.1186/1748-7161-5-16.
There are a number of reasons for intraoperative blood loss during scoliosis surgery based on the type of approach, type of disease, osteopenia, and patient blood profile. However, no studies have investigated bleeding patterns according to the stage of the operation. The objective of this prospective study was to identify intraoperative bleeding patterns in different stages of scoliosis surgery.
We prospectively analyzed the estimated blood loss (EBL) and operation time over four stages of scoliosis surgery in 44 patients. The patients were divided into three groups: adolescent idiopathic (group 1), spastic neuromuscular (group 2) and paralytic neuromuscular (group 3). The per-level EBL and operation times of the groups were compared on a stage-by-stage basis. The bone marrow density (BMD) of each patient was also obtained, and the relationship between per-level EBL and BMD was compared using regression analysis.
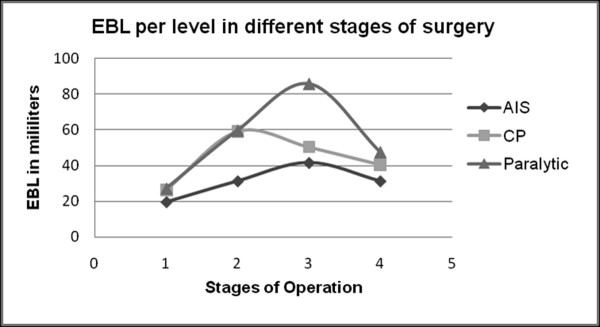
Per-level operation time was similar across all groups during surgical stage (p > 0.05). Per-level EBL was also similar during the dissection and bone-grafting states (p > 0.05). However, during the screw insertion stage, the per-level EBL was significantly higher in groups 2 and 3 compared to group 1 (p < 0.05). In the correction stage, per-level EBL was highest in group 3 (followed in order by groups 2 and 1) (p < 0.05). Preoperative BMD indicated that group 3 had the lowest bone quality, followed by groups 2 and 1 (in order), but the preoperative blood indices were similar in all groups. The differences in bleeding patterns in the screw insertion and correction stages were attributed to the poor bone quality of groups 2 and 3. Group 3 had the lowest bone quality, which caused loosening of the bone-screw interface during the correction stage and led to more bleeding. Patients with a T-score less than -2.5 showed a risk for high per-level EBL that was nine times higher than those with scores greater than -2.5 (p = 0.003).
We investigated the blood loss patterns during different stages of scoliosis surgery. Patients with poor BMD showed a risk of blood loss nine times higher than those with good BMD.
基于手术入路类型、疾病类型、骨质减少和患者血液状况等因素,脊柱侧弯手术中存在多种导致术中失血的原因。然而,尚无研究根据手术阶段来调查出血模式。这项前瞻性研究的目的是确定脊柱侧弯手术不同阶段的术中出血模式。
我们前瞻性分析了44例患者在脊柱侧弯手术四个阶段的估计失血量(EBL)和手术时间。患者分为三组:青少年特发性(第1组)、痉挛性神经肌肉型(第2组)和麻痹性神经肌肉型(第3组)。对各组每节段的EBL和手术时间进行逐阶段比较。还获取了每位患者的骨髓密度(BMD),并使用回归分析比较每节段EBL与BMD之间的关系。
在手术阶段,所有组每节段的手术时间相似(p>0.05)。在解剖和植骨阶段,每节段的EBL也相似(p>0.05)。然而,在螺钉置入阶段,第2组和第3组每节段的EBL显著高于第1组(p<0.05)。在矫正阶段,第3组每节段的EBL最高(其次依次为第2组和第1组)(p<0.05)。术前BMD显示第3组骨质质量最低,其次依次为第2组和第1组,但所有组术前血液指标相似。螺钉置入和矫正阶段出血模式的差异归因于第2组和第3组骨质质量差。第3组骨质质量最低,这导致在矫正阶段骨螺钉界面松动并导致更多出血。T评分小于-2.5的患者每节段EBL高风险比评分大于-2.5的患者高9倍(p=0.003)。
我们调查了脊柱侧弯手术不同阶段的失血模式。BMD差的患者失血风险比BMD好的患者高9倍。