Division of Radiation Oncology, H. Lee Moffitt Cancer Center, Tampa, Florida 33612, USA.
J Appl Clin Med Phys. 2010 Jun 15;11(3):3240. doi: 10.1120/jacmp.v11i3.3240.
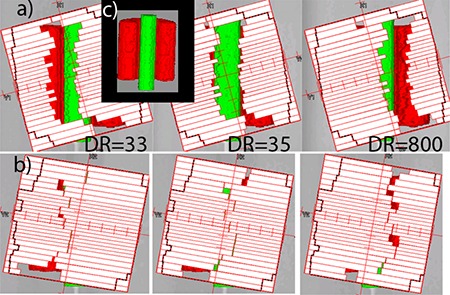
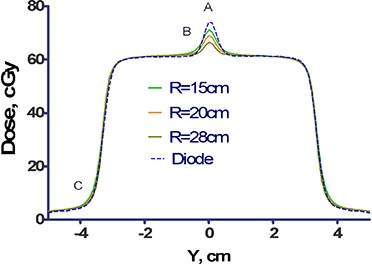
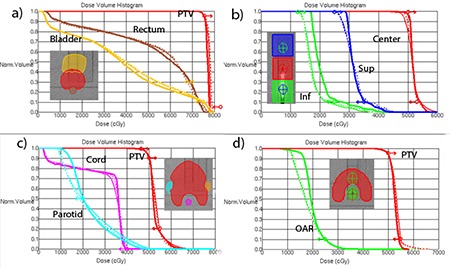
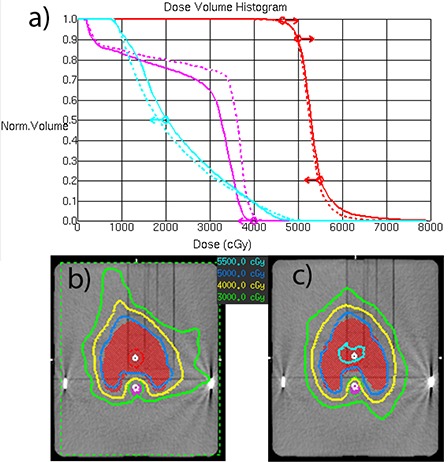
For an institution that already owns the licenses, it is economically advantageous and technically feasible to use Pinnacle TPS (Philips Radiation Oncology Systems, Fitchburg, WI) with the BrainLab Novalis delivery system (BrainLAB A.G., Heimstetten, Germany). This takes advantage of the improved accuracy of the convolution algorithm in the presence of heterogeneities compared with the pencil beam calculation, which is particularly significant for lung SBRT treatments. The reference patient positioning DRRs still have to be generated by the BrainLab software from the CT images and isocenter coordinates transferred from Pinnacle. We validated this process with the end-to-end hidden target test, which showed an isocenter positioning error within one standard deviation from the previously established mean value. The Novalis treatment table attenuation is substantial (up to 6.2% for a beam directed straight up and up to 8.4% for oblique incidence) and has to be accounted for in calculations. A simple single-contour treatment table model was developed, resulting in mean differences between the measured and calculated attenuation factors of 0.0%-0.2%, depending on the field size. The maximum difference for a single incidence angle is 1.1%. The BrainLab micro-MLC (mMLC) leaf tip, although not geometrically round, can be represented in Pinnacle by an arch with satisfactory dosimetric accuracy. Subsequently, step-and-shoot (direct machine parameter optimization) IMRT dosimetric agreement is excellent. VMAT (called "SmartArc" in Pinnacle) treatments with constant gantry speed and dose rate are feasible without any modifications to the accelerator. Due to the 3 mm-wide mMLC leaves, the use of a 2 mm calculation grid is recommended. When dual arcs are used for the more complex cases, the overall dosimetric agreement for the SmartArc plans compares favorably with the previously reported results for other implementations of VMAT: gamma(3%,3mm) for absolute dose obtained with the biplanar diode array passing rates above 97% with the mean of 98.6%. However, a larger than expected dose error with the single-arc plans, confined predominantly to the isocenter region, requires further investigation.
对于已经拥有许可证的机构,使用配备 BrainLab Novalis 交付系统的 Pinnacle TPS(飞利浦放射肿瘤系统,美国威斯康星州菲奇堡)具有经济优势并且在技术上也是可行的,这种方式利用了卷积算法在存在异质性时比铅笔束计算具有更高的准确性,这对于肺部 SBRT 治疗尤其重要。参考患者定位 DRR 仍然需要由 BrainLab 软件从 CT 图像和从 Pinnacle 传输的等中心坐标生成。我们使用端到端隐藏目标测试验证了该过程,该测试显示等中心定位误差在之前建立的平均值的一个标准差范围内。Novalis 治疗床衰减量很大(对于直接向上的射束可达 6.2%,对于斜入射可达 8.4%),在计算中必须考虑到这一点。开发了一种简单的单轮廓治疗床模型,结果表明,测量和计算衰减因子之间的平均差异在 0.0%至 0.2%之间,具体取决于射野大小。对于单个入射角的最大差异为 1.1%。BrainLab 微多叶准直器(mMLC)叶尖虽然不是几何圆形的,但可以在 Pinnacle 中用一个拱门来表示,具有令人满意的剂量学准确性。随后,直接机器参数优化的步进和射击(step-and-shoot)调强适形放疗剂量学一致性非常好。对于没有对加速器进行任何修改的情况下,恒剂量率和恒机架速度的容积调制弧形治疗(在 Pinnacle 中称为“SmartArc”)是可行的。由于 mMLC 叶片的宽度为 3 毫米,建议使用 2 毫米的计算网格。对于更复杂的情况,使用双弧时,SmartArc 计划的整体剂量学一致性与其他 VMAT 实现报告的结果相比具有优势:使用双平面二极管阵列获得的绝对剂量的γ(3%,3mm)通过率超过 97%,平均值为 98.6%。但是,单弧计划中存在比预期更大的剂量误差,主要集中在等中心区域,需要进一步调查。