Department of Pediatrics, Monash University, Monash Newborn, Monash Medical Centre, Monash Institute for Medical Research, 246 Clayton RD, Clayton 3168, Melbourne, Australia.
Crit Care. 2010;14(4):R156. doi: 10.1186/cc9226. Epub 2010 Aug 19.
Purpura fulminans (PF) is a devastating complication of uncontrolled systemic inflammation, associated with high incidence of amputations, skin grafts and death. In this study, we aimed to clarify the clinical profile of pediatric patients with PF who improved with protein C (PC) treatment, explore treatment effects and safety, and to refine the prognostic significance of protein C plasma levels.
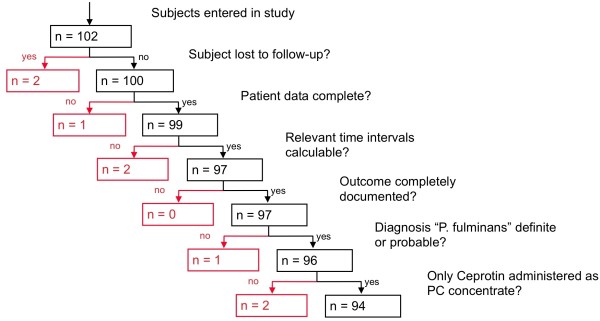
In Germany, patients receiving protein C concentrate (Ceprotin, Baxter AG, Vienna, Austria) are registered. The database was used to locate all pediatric patients with PF treated with PC from 2002 to 2005 for this national, retrospective, multi-centered study.
Complete datasets were acquired in 94 patients, treated in 46 centers with human, non-activated protein C concentrate for purpura fulminans. PC was given for 2 days (median, range 1-24 days) with a median daily dose of 100 IU/kg. Plasma protein C levels increased from a median of 27% to a median of 71% under treatment. 22.3% of patients died, 77.7% survived to discharge. Skin grafts were required in 9.6%, amputations in 5.3%. PF recovered or improved in 79.8%, remained unchanged in 13.8% and deteriorated in 6.4%. Four adverse events occurred in 3 patients, none classified as severe. Non-survivors had lower protein C plasma levels (P < 0.05) and higher prevalence of coagulopathy at admission (P < 0.01). Time between admission and start of PC substitution was longer in patients who died compared to survivors (P = 0.03).
This retrospective dataset shows that, compared to historic controls, only few pediatric patients with PF under PC substitution needed dermatoplasty and/or amputations. Apart from epistaxis, no bleeding was observed. Although the data comes from a retrospective study, the evidence we present suggests that PC had a beneficial impact on the need for dermatoplasty and amputations, pointing to the potential value of carrying out a prospective randomised controlled trial.
暴发性紫癜(PF)是一种严重的全身性炎症失控并发症,其高发生率与截肢、植皮和死亡有关。本研究旨在阐明接受蛋白 C(PC)治疗后病情改善的小儿暴发性紫癜患者的临床特征,探讨治疗效果和安全性,并进一步明确蛋白 C 血浆水平的预后意义。
在德国,接受蛋白 C 浓缩物(Ceprotin,Baxter AG,维也纳,奥地利)治疗的患者都需进行登记。本研究通过使用该数据库,从 2002 年至 2005 年期间定位了所有接受 PC 治疗的暴发性紫癜患儿,这是一项全国性、回顾性、多中心研究。
共纳入 94 例患儿,这些患儿在 46 个中心接受了人源性非激活蛋白 C 浓缩物治疗暴发性紫癜。PC 治疗持续 2 天(中位数,范围 1-24 天),每日剂量中位数为 100IU/kg。治疗期间,血浆蛋白 C 水平从中位数 27%增加至中位数 71%。22.3%的患者死亡,77.7%存活至出院。9.6%的患者需要植皮,5.3%的患者需要截肢。79.8%的患者暴发性紫癜恢复或改善,13.8%的患者病情无变化,6.4%的患者病情恶化。3 例患儿出现 4 例不良事件,均未归类为严重不良事件。非幸存者的蛋白 C 血浆水平较低(P<0.05),入院时凝血障碍的发生率较高(P<0.01)。与幸存者相比,死亡患者接受 PC 替代治疗的时间更长(P=0.03)。
本回顾性数据集表明,与历史对照相比,接受 PC 替代治疗的暴发性紫癜患儿中,仅有少数需要植皮和/或截肢。除鼻出血外,未观察到其他出血情况。虽然这些数据来自回顾性研究,但我们提供的证据表明,PC 治疗对植皮和截肢的需求有有益影响,这表明进行前瞻性随机对照试验具有潜在价值。