Mobayed Mohammad, Heilbrun Lance K, Shields Anthony F, Washington Tara, Venkatramanamoorthy Raghu, Philip Philip A, El-Rayes Bassel F
Division of Hematology/Oncology, Karmanos Cancer Institute, Detroit, Mich., USA.
Case Rep Oncol. 2009 Nov 21;2(3):220-228. doi: 10.1159/000250082.
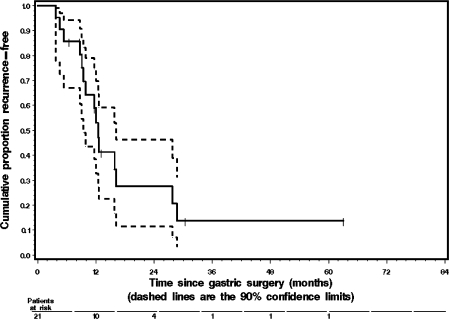
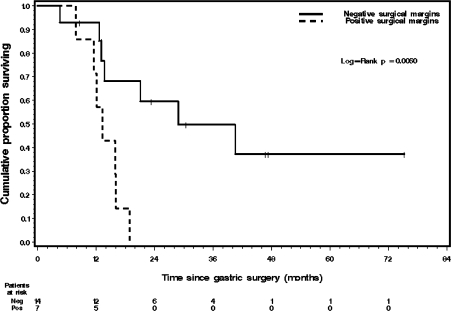
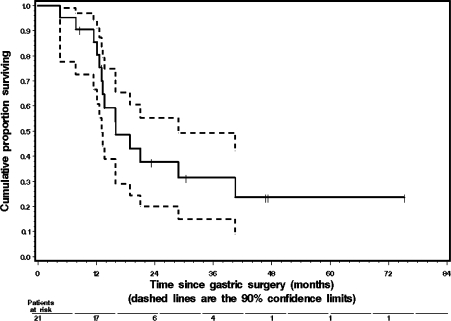
Adjuvant 5-fluorouracil (5FU)-based chemo-radiotherapy is currently considered a standard of care for the treatment of gastric cancer. The impact of 5FU-based adjuvant therapy on the rate of distant recurrence has been modest. In order to improve the systemic effects of adjuvant therapy, we have been treating patients with resected gastric cancer with carboplatin and paclitaxel followed by fluoropyrimidine analogue and radiation. METHODS: We report on the outcomes of 21 consecutive gastric cancer patients treated off protocol with adjuvant carboplatin (area under the curve 5 mg/ml x min) and paclitaxel (175-200 mg/m(2)) every 3 weeks, followed by concurrent pyrimidine analogs (either capecitabine 1,600-2,000 mg/m(2)/day in 17 patients, or 5FU 200 mg/m(2)/day in 4 patients) and radiation (45-50.4 Gy). Patients received a total of 4-6 cycles of carboplatin and paclitaxel. RESULTS: The median age at diagnosis was 60 years. Sixteen patients had stage 3 disease and 7 of them had positive surgical margins (6 with R1 and 1 with R2 resection), 3 patients were stage 2, and 2 patients were stage 1 (all had R0 resection). All patients had D1/D2 (4 had D2 and 17 had D1) lymph node dissection. The incidence of grade 3 or higher overall, hematologic, or gastrointestinal toxicity in the patients receiving carboplatin and paclitaxel was 57, 48 and 10%, respectively. No treatment-related deaths were observed. After adjuvant treatment 15 patients developed recurrent disease, 10 of whom had distant metastases. The median recurrence-free survival (RFS) was 12.3 months. The median overall survival (OS) was 16.0 months. Patients with R0 resection had significantly longer OS than did those with positive surgical margins (log-rank p = 0.0060). Median OS for the R0 resection group was 28.8 months. CONCLUSIONS: Carboplatin and paclitaxel added to radiation plus fluoropyrimidine analogs is a well-tolerated regimen in the adjuvant setting. The activity of this regimen in this relatively high-risk group of gastric cancer patients is of interest for future development.
基于氟尿嘧啶(5FU)的辅助放化疗目前被认为是胃癌治疗的标准疗法。基于5FU的辅助治疗对远处复发率的影响不大。为了提高辅助治疗的全身效果,我们一直采用卡铂和紫杉醇治疗接受胃癌切除术的患者,随后给予氟嘧啶类似物和放疗。
我们报告了21例连续接受非方案辅助治疗的胃癌患者的结果,每3周给予卡铂(曲线下面积5mg/ml×min)和紫杉醇(175 - 200mg/m²),随后给予嘧啶类似物(17例患者给予卡培他滨1600 - 2000mg/m²/天,4例患者给予5FU 200mg/m²/天)和放疗(45 - 50.4Gy)。患者共接受4 - 6周期的卡铂和紫杉醇治疗。
诊断时的中位年龄为60岁。16例患者为3期疾病,其中7例手术切缘阳性(6例为R1切除,1例为R2切除),3例患者为2期,2例患者为1期(均为R0切除)。所有患者均行D1/D2(4例为D2,17例为D1)淋巴结清扫。接受卡铂和紫杉醇治疗的患者中,3级或更高的总体、血液学或胃肠道毒性发生率分别为57%、48%和10%。未观察到与治疗相关的死亡。辅助治疗后,15例患者出现复发疾病,其中10例发生远处转移。中位无复发生存期(RFS)为12.3个月。中位总生存期(OS)为16.0个月。R0切除的患者OS明显长于手术切缘阳性的患者(对数秩检验p = 0.0060)。R0切除组的中位OS为28.8个月。
在辅助治疗中,卡铂和紫杉醇联合放疗加氟嘧啶类似物是一种耐受性良好的方案。该方案在这一相对高危的胃癌患者群体中的活性值得未来进一步研究。